

Introduction
When a poisoned patient comes to the OPD, the individual does not come in with a premeditated label of a toxin. It is an organism under pharmacological stress whose vital signs, mental status, pupils, skin, and neuromuscular tone form this repertoire of molecular injury that the clinician must recognize. Clinical toxicology fails when it defers management to the toxicology screening and waits for the results, while the patient might slip into the abyss of physiological dysfunction. Success is only true when it enables prompt management before any laboratory confirmation, before any screening that might be too slow, too passive and too ambiguous to detect anything meaningful within the critical window. The way of thinking, “treat the threat to physiology first”, makes the clinician the interpreter rather than a toxin identifier, recognizing that most poisons kill through a small number of final common pathways: respiratory depression, cardiovascular collapse, seizure, liver and renal dysfunction, and thermal dysregulation.
The Syndromic Language of Poison
Toxidromes are not just some nightmarish mnemonics in the lives of medical students. They are the clinical signatures of receptor-level pharmacology expressed through the autonomic nervous system, and correctly interpreting them requires quintessential understanding of the mechanisms underlying each pattern.
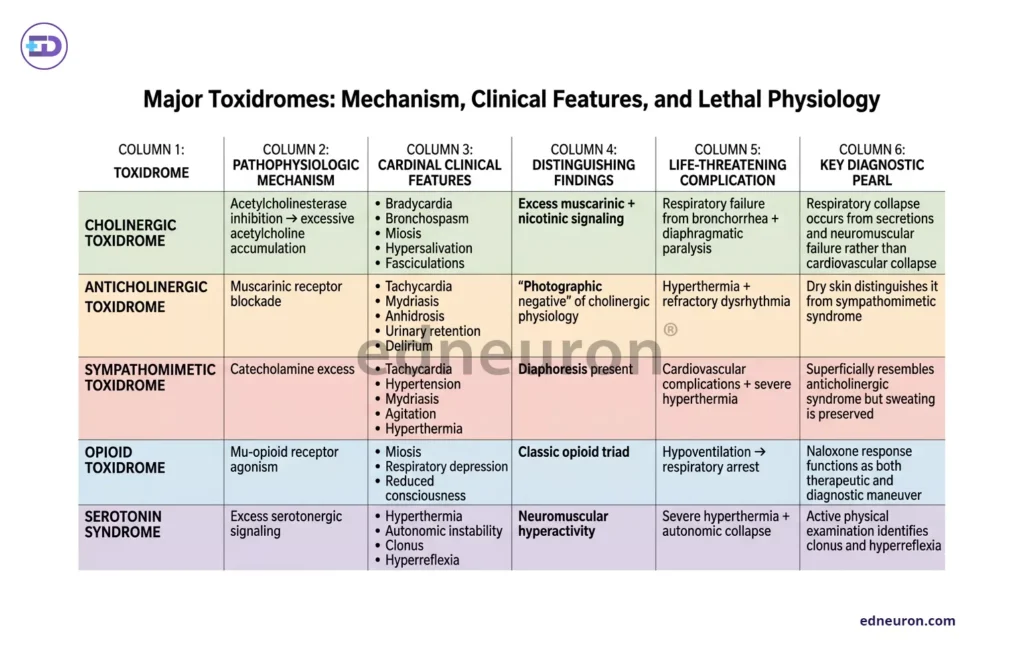
Table 1 : Various toxidromes and their pathognomic patterns of clinical presentation and findings.
The cholinergic toxidrome: unbridled acetylcholine accumulation from acetylcholinesterase inhibition; its lethal endpoint is respiratory failure from bronchorrhea and diaphragmatic paralysis, not cardiovascular collapse.
Symptoms: bradycardia, bronchospasm, miosis, hypersalivation, and fasciculations.
The anticholinergic toxidrome is its photographic negative produced by muscarinic receptor blockade and becomes lethal through hyperthermia and refractory dysrhythmia.
Symptoms: tachycardia, mydriasis, anhidrosis, urinary retention, and delirium.
The sympathomimetic syndrome mimics anticholinergic physiology superficially but is distinguished by diaphoresis and, crucially, by its catecholamine-driven mechanism, which predicts both the treatment response and the cardiovascular complications.
Opioid toxidrome: It is caused by overstimulatory mu-receptor agonistic activity that results in a triad of miosis, respiratory depression, and reduced consciousness. Its elegant reversibility with naloxone is itself a diagnostic test as well as a therapeutic treatment.
Serotonin syndrome occupies a peculiar, distinct, and frequently missed niche: the triad of autonomic instability, hyperthermia, and neuromuscular hyperactivity (clonus, hyperreflexia), which reflects excessive serotonergic signaling and demands active physical examination to distinguish it from the sedated, areflexic patient.
When Laboratories Lag Behind Physiology
Urine toxicology immunoassays are approximations, not toxicological diagnoses. The problems with these assays are:
- They cover a narrow pharmacological range.
- Fail to detect most synthetic opioids and novel psychoactive substances.
- Generate false positives with clinical regularity.
More fundamentally, the existing tests are qualitative rather than quantitative, as evidently proven when a positive opioid screen does not explain unconsciousness, and a negative amphetamine screen does not exclude sympathomimetic poisoning. With a better understanding of acetaminophen kinetics, risk stratification, and wider availability of lab tests to get prompt results, the NACSTOP trial devised a newer regimen for antidotal therapy. A complete two-bag acetylcysteine regimen was administered in 12 hours rather than the conventional 20-hour 3-bag regimen, and zero trial subjects reported hepatic injury and adverse effects on follow-up. Carbon monoxide poisoning is routinely missed because standard pulse oximetry cannot distinguish carboxyhemoglobin from oxyhemoglobin, and the diagnosis requires co-oximetry that must be actively requested. Mixed overdoses with 85% of MDMA cases co-positive for other substances which constitute the majority of presentations in real-world practice, produce blended or antagonistically canceled toxidromes where no single pattern is legible without understanding the receptor-level mechanism of each co-ingested agent. Bedside clinical reasoning, anchored in physiologic pattern recognition, remains the most temporally appropriate diagnostic tool available.
Principles of Management:
The clinical management of the poisoned patient follows a hierarchy practiced and codified for generations: secure the patient before pursuing the poison, and address systemic derangement before source attribution. The primary survey: airway patency, respiratory adequacy, circulatory stability, and conscious level, must precede every other intervention. We call this the ABC of poisoning management–Airway, Breathing and Circulation. An obstructed airway from a sedative overdose can kill before the toxicology result from the lab returns; endotracheal intubation must be prioritized before anything.
- Gastric decontamination which was once reflexively applied, is now understood as an intervention with a narrow, rapidly closing temporal window. However, special cases like corrosive ingestion, petroleum products, and any patient with altered consciousness, induced emesis is contraindicated as it increases the risk of aspiration and mucosal re-injury. Gastric lavage, when performed, requires strict attention to airway protection and is most effective within 1 hour of ingestion; beyond that, its use is not supported by evidence. Activated charcoal-the single most broadly applicable decontaminant for oral ingestion-acts on the principle of adsorptive surface binding and is effective within one to two hours for most xenobiotics. We use multidose activated charcoal for compounds that undergo enterohepatic circulation, such as carbamazepine and theophylline.
- Antidotes for specific drugs should be deployed without delay whenever and wherever available.
Atropine in organophosphate poisoning competes at the muscarinic receptor and should be titrated to drying of secretions (signs of atropinization) rather than heart rate, since inadequate atropinization is the primary cause of preventable death in cholinergic crisis. Pralidoxime (PAM), which reactivates acetylcholinesterase (not used in carbamate poisoning) must be employed before aging (dealkylation) of the enzyme-inhibitor bond renders it irreversible, and its early administration, ideally within 4 to 6 hours, is time-critical in a mechanistically derived, not arbitrary, way.
N-acetylcysteine given at a dose of 300mg/kg over 20 hours or 12 hours, depending on risk stratification for acetaminophen hepatotoxicity, replenishes glutathione stores, thus reducing free radical stress before the metabolite NAPQI accumulates to a hepatocellular lethal concentration. The Rumack-Matthew nomogram provides the pharmacokinetic framework for initiation values.
Naloxone given for opioid toxicity, flumazenil in benzodiazepine overdose, calcium and high-dose insulin euglycemia therapy for CCB (calcium channel blocker) toxicity, and hydroxocobalamin in cyanide poisoning each converges at the very same philosophy wherein the antidote is rational and of utmost importance when its molecular target is identified, and its deployment is time-appropriate. - Supportive care cannot and should not be an afterthought because it forms the very backbone of poisoning management. Fluid resuscitation, vasopressors in refractory hypotension, benzodiazepines for toxin-driven seizure, and aggressive cooling in hyperthermia become the very lexicon, especially when no specific antidote exists. Special methods for eliminating toxic metabolites, such as enhanced excretion through urinary alkalinization (salicylates, phenobarbital) using sodium barcarbonate and potassium citrate or extracorporeal removal via hemodialysis, plasmapheresis, or hemoperfusion, expand the toolkit for agents that meet the pharmacokinetic criteria of low molecular weight, low protein binding, small volume of distribution, and water solubility. To escalate to such treatment, the decision should be based on careful evaluation and anchored in severity thresholds, toxin concentrations, metabolic derangement analysis, and end-organ dysfunction.
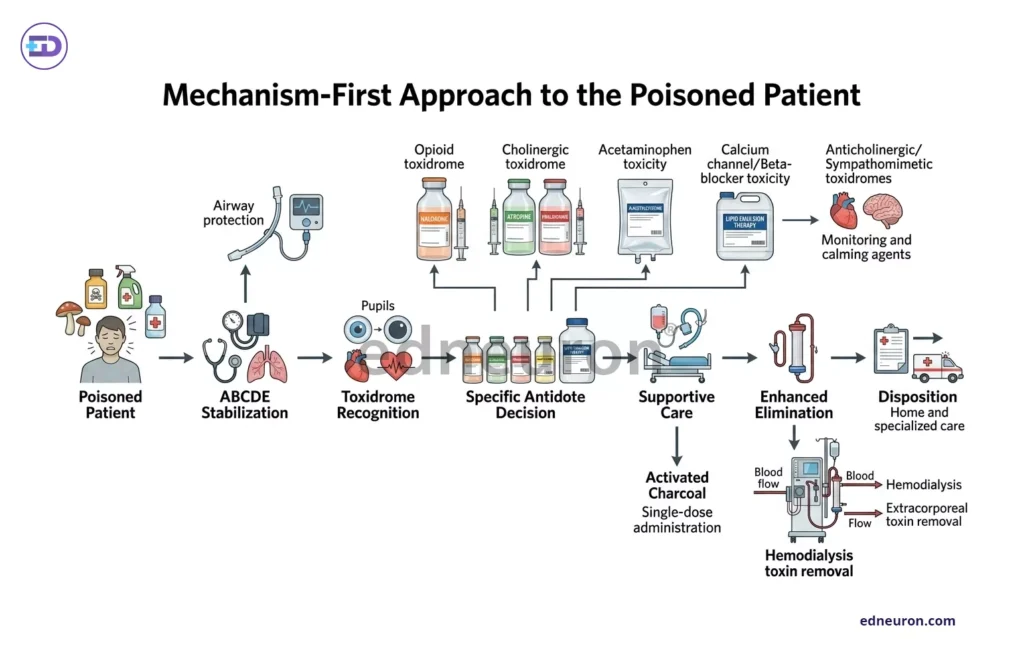
Fig 1 : Stepwise algorithm to managing a patient with posioning.
Modern Toxicology Beyond Ritual
Three decades of evidence have eroded the ritual decontamination algorithms of earlier toxicology. Activated charcoal with its historical legacy, retains some of its original value for its adsorptive capacity, but within a strict pharmacokinetics framework, its utility is meaningful only when administered within one to two hours of ingestion of a charcoal-amenable substance, with an intact airway. It is proven ineffective in substances such as metals, alcohols, and caustics. Gastric lavage has retreated to being nothing more than a historical footnote outside of narrowly defined life-threatening scenarios. Intravenous lipid emulsion therapy, first described for bupivacaine cardiotoxicity in 1998, has expanded pragmatically through its lipid-sink mechanism, increased mitochondrial fatty acid uptake, reduced interaction with sodium voltage channels, attenuation of endothelium nitric oxide and increased liver shunting. It sequesters lipophilic drugs in a newly created plasma compartment, drawing them and preventing their entry into tissues, providing buffer time for their elimination and metabolism. We have seen promising results, as evidenced by its use with tricyclic antidepressants, calcium channel blockers, and other highly lipid-soluble xenobiotics, though rigorous trial data remain sparse.
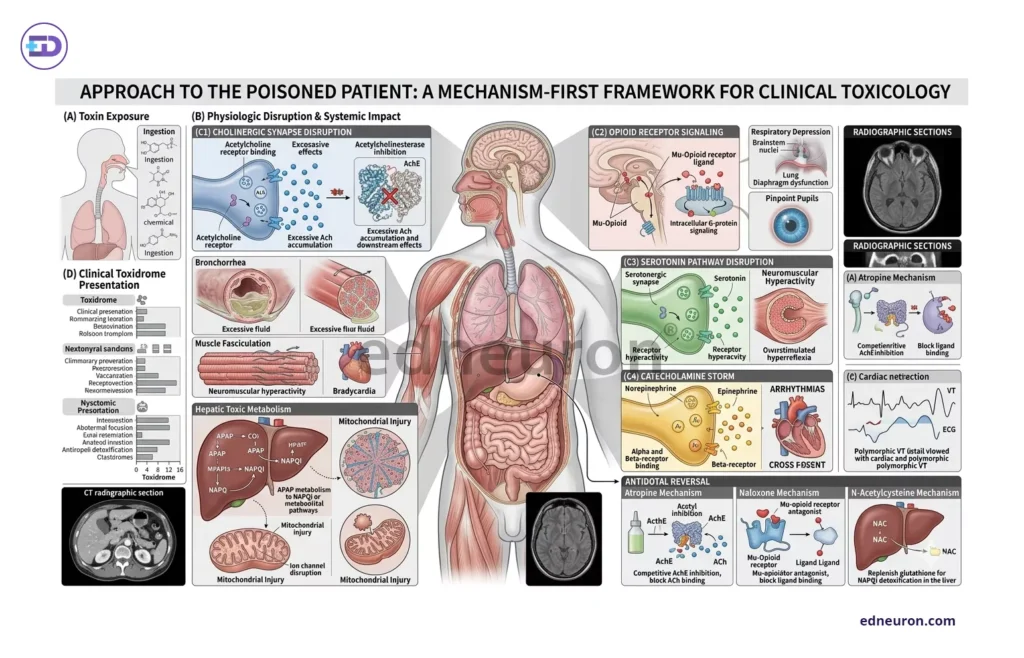
Fig 2 : Toxidrome approach to poisoning patient.
Conclusion
A poisoned patient cannot afford any delay in active initiation of management. It must come as a realization that laboratory investigations confirm, quantify, and prognosticate; they do not initiate management in the critically ill. The patient should be the priority before anything else and must be stabilized, followed by a thorough, systematic evaluation assessing pupillary response, autonomic tone, neuromuscular activity, mental status, and skin findings to provide a receptor-level diagnosis within minutes of presentation. Modern toxicology’s advances succeed because they are engineered to match the pharmacokinetic and pharmacodynamic principles of the disrupted pharmacology rather than being applied empirically. Poisoning management is, at its core, recognition of subversion of physiology, whose recovery depends on restoring those systems faster before the toxin plagues the entire system.
References
- Jaffal K, Chevillard L, Mégarbane B. Lipid Emulsion to Treat Acute Poisonings: Mechanisms of Action, Indications, and Controversies. Pharmaceutics. 2023 May 3;15(5):1396. PMID: 37242638.
- Nelson LS, Howland MA, Lewin NA, et al. Goldfrank’s Toxicologic Emergencies. 11th ed. New York: McGraw-Hill; 2022.
- General Principles of Poisoning. MSD Manuals Professional Version. Merck & Co.; 2025 [cited 2026 May 24]. Available from: https://www.msdmanuals.com/professional/injuries-poisoning/poisoning/general-principles-of-poisoning
- Wong, Anselm & McNulty, Richard & Taylor, David & Sivilotti, Marco & Greene, Shaun & Gunja, Naren & Koutsogiannis, Zeff & Graudins, Andis. (2018). The NACSTOP Trial: A Multicenter, Cluster-Controlled Trial of Early Cessation of Acetylcysteine in Acetaminophen Overdose. Hepatology. 69. 10.1002/hep.30224.
- Reddy KSN. The Essentials of Forensic Medicine and Toxicology. 34th ed. Hyderabad: K. Suguna Devi; 2017.

Author: Edneuron Admin
testing
