Introduction
Hansen’s disease is a chronic infection that has existed for centuries, yet it still poses a major diagnostic challenge today. Even though the World Health Organization’s “Toward Zero Leprosy” initiative has set ambitious goals, there remains a significant gap in recognizing the disease in real-world practice. The main problem is that the classic “cardinal signs” of leprosy often do not match how the disease actually appears, since it can imitate many other skin and nerve conditions. Because the bacteria grow slowly and interact in complex ways with the immune system, leprosy often appears as more common dermatological or neurological problems rather than the textbook case.
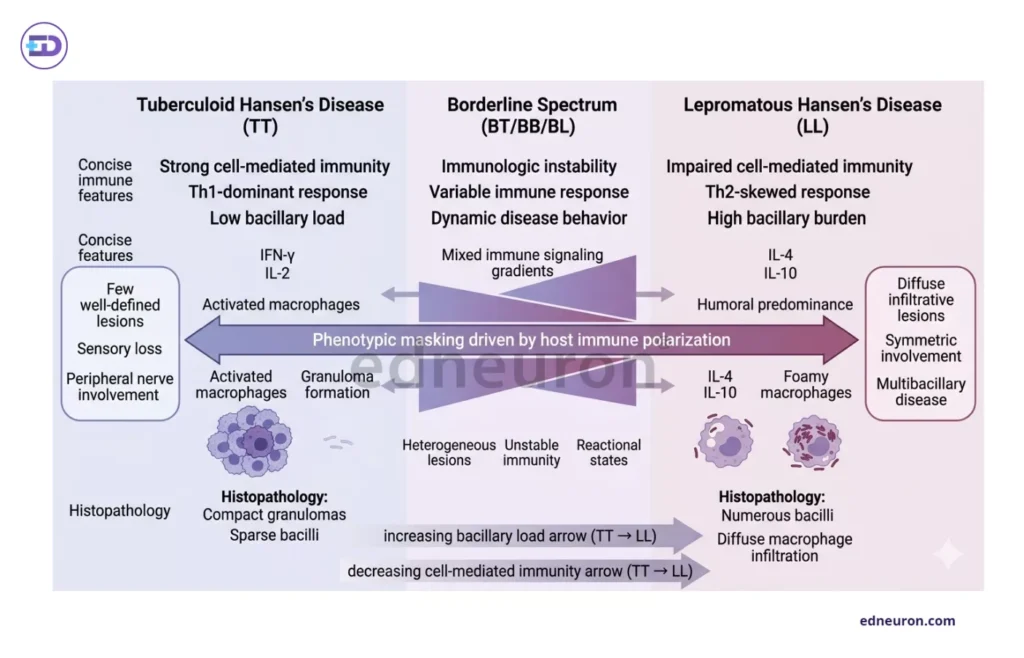
Fig 1: Host immune polarization determines the phenotypic spectrum and diagnostic variability of Hansen’s disease.
The Immunological Veil: Pathophysiology as a Phenotypic Mask
Leprosy does not always look the same; its appearance depends on the patient’s immune response. In tuberculoid leprosy (TT), a strong Th1 immune response keeps the bacteria contained, so doctors may see only one small lesion that tests negative on a smear and shows no clear nerve thickening. On the other hand, in lepromatous leprosy (LL), a weak Th2 response allows the bacteria to multiply unchecked, leading to widespread thickening, nodules, or plaques that can resemble common warts or calluses.
This leads to an important question: if the immune response shapes how leprosy looks, can we really depend on the classic “cardinal signs” to catch it early? M. leprae targets Schwann cells and the reticuloendothelial system, so nerve damage often starts before any clear loss of sensation appears. To make things harder, about 70% of leprosy cases—especially those with few bacteria—have negative skin slit smears. This means the most reliable sign is often missing when early treatment would be most helpful
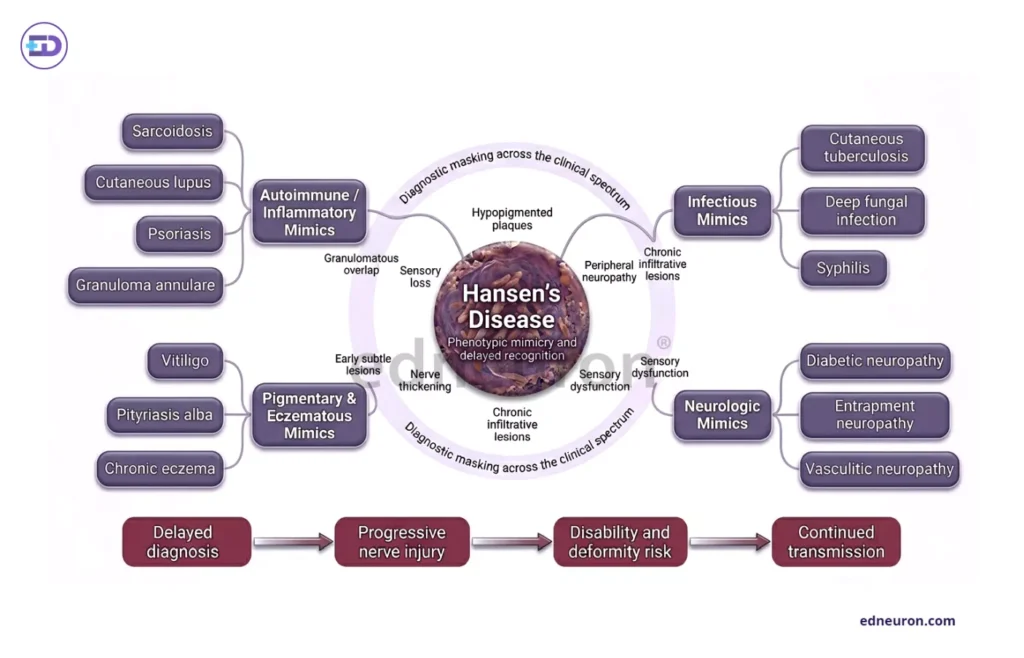
Fig 2 : Phenotypic mimicry in Hansen’s disease contributes to delayed recognition, diagnostic misclassification, and progressive neurologic injury.
The Failure of Recognition: When Mimicry Becomes Misdiagnosis
Doctors often get stuck focusing on more common diagnoses, a problem sometimes called “interpretive inertia.” Hansen’s disease can easily be mistaken for conditions like sarcoidosis, psoriasis, or lupus. One reason new cases are still found at a high rate, even though overall prevalence is down, is that many cases are missed until the disease becomes severe or causes sudden reactions.
For example, elevated serum Angiotensin-Converting Enzyme (ACE), which is usually indicative of sarcoidosis, can also be seen in leprosy. This can result in patients getting corticosteroids for too long while the real infection goes untreated. Leprosy can also look just like juvenile idiopathic arthritis or rheumatoid arthritis, especially when patients suddenly develop swelling and nerve pain in their limbs.
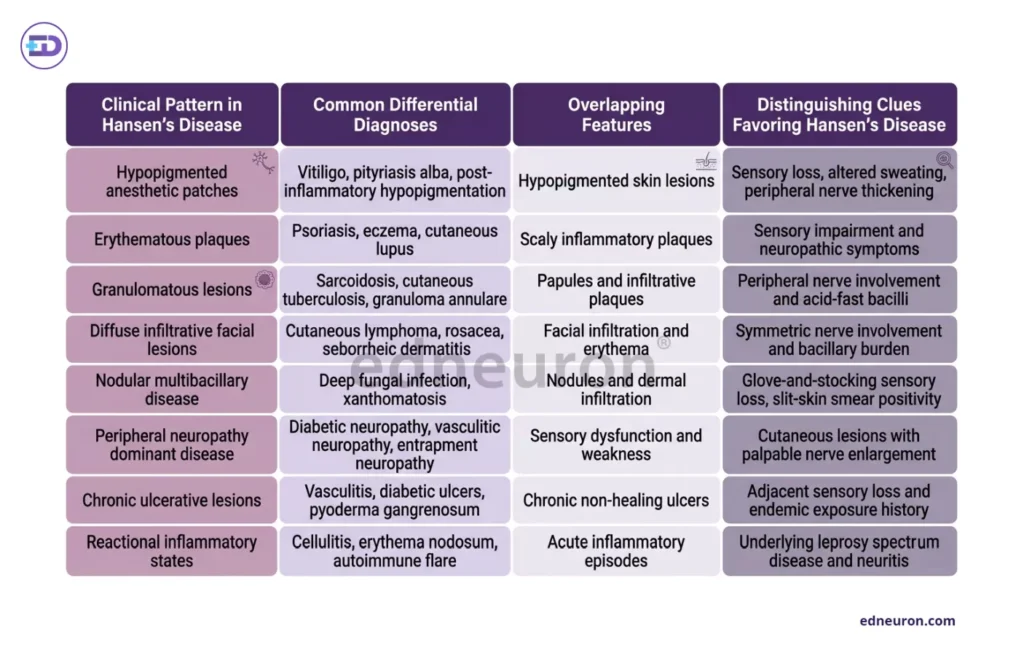
Table 1 : Key differential diagnoses across the leprosy spectrum, highlighting clinical overlap and distinguishing diagnostic clues favoring Hansen’s disease.
Delaying diagnosis does more than let a rash linger—it can lead to permanent Grade 2 Disabilities (G2D). Catching leprosy early is the only way to stop its spread and prevent the physical changes that cause social stigma. The risk is even greater for children, since high rates in those under 15 mean the disease is still spreading in the community. Treating children is also harder because there are no easy-to-use oral medicines for them, and long-term treatment can be difficult for families. This makes a family-centered, holistic approach to care essential.
Conclusion
The evidence does not give us an easy answer, but it does show the need for constant clinical awareness. Managing Hansen’s disease is less about lab tests, which are often limited or unavailable, and more about keeping a high level of suspicion, even when the case does not look like the textbook example. In both high- and low-risk areas, a non-healing lesion with slight sensory changes should not be seen as just an odd case; it is a medical emergency. The chance to change a patient’s life depends on the clinician’s willingness to look beyond the obvious.
References
- Bhat RM, Prakash C. Leprosy: an overview of pathophysiology. Dermatol Res Pract. 2012;2012:181089. doi:10.1155/2012/181089. PMID: 22888457; PMCID: PMC3440852.
- Moschella SL. An update on the diagnosis and treatment of leprosy. J Am Acad Dermatol. 2004;51(3):417-426. doi:10.1016/j.jaad.2003.11.1069. PMID: 15337986.
- Frade MAC, de Paula NA, Gomes CM, Vernal S, Bernardes Filho F. Leprosy: clinical and immunopathological characteristics. An Bras Dermatol. 2022;97(3):338-347. doi:10.1016/j.abd.2021.08.006. PMID: 35007803; PMCID: PMC9133310.
- Mikhaylov D, Salman A, Heisler M, et al. Hansen’s disease: a practical update on a neglected globally significant infection. Cureus. 2024;16(3):e56492. doi:10.7759/cureus.56492. PMID: 38601554; PMCID: PMC11026725.
- Nguyen K, Patel V, Cockerell CJ, Husain S. Extensor plaques with associated arthritis and neuropathy. JAAD Case Rep. 2020;6(8):748-751. doi:10.1016/j.jdcr.2020.06.018. PMID: 32715266; PMCID: PMC7355211.
- Muteba M, Mvumbi DM, Mbuyi-Musanzayi S, et al. Diagnostic difficulty: an elusive case of Hansen’s disease mimicking sarcoidosis. PAMJ Clin Med. 2020;2:122. doi:10.11604/pamj-cm.2020.2.122.22977.
- Ribeiro de Castro MC, Ianhez M, Miot HA. Verrucous form of Hansen disease: a diagnostic dilemma. Skin Health Dis. 2025;6(2):vzaf114. doi:10.1093/skinhd/vzaf114. PMID: 40184979; PMCID: PMC11925335.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India