Introduction
Psoriasis is typically easy to spot because it appears symmetrically on the outer parts of the body. However, when it affects just one sensitive area, diagnosing it becomes much harder. The biggest challenge is telling the difference between a harmless skin condition and serious cancers like Paget’s disease of the breast or inflammatory breast cancer. This article presents a case of long-standing psoriasis on one breast to show how unusual locations can delay both diagnosis and treatment.
Case Presentation
A woman in her late 60s arrived with a three-year history of a single, painful, scaly patch on her left breast. The area was red, had sores, and felt warmer than her other breast. Despite its appearance, she had no other symptoms, no nipple discharge, and no family history of cancer.
Before seeing a specialist, the patient tried antibiotics, antifungal creams, and steroid creams for three years, but none helped. Both a 3D mammogram and an X-ray were normal, yet the patch sustained. A full skin exam found no other typical psoriasis spots on her scalp, elbows, knees, or between the buttocks.
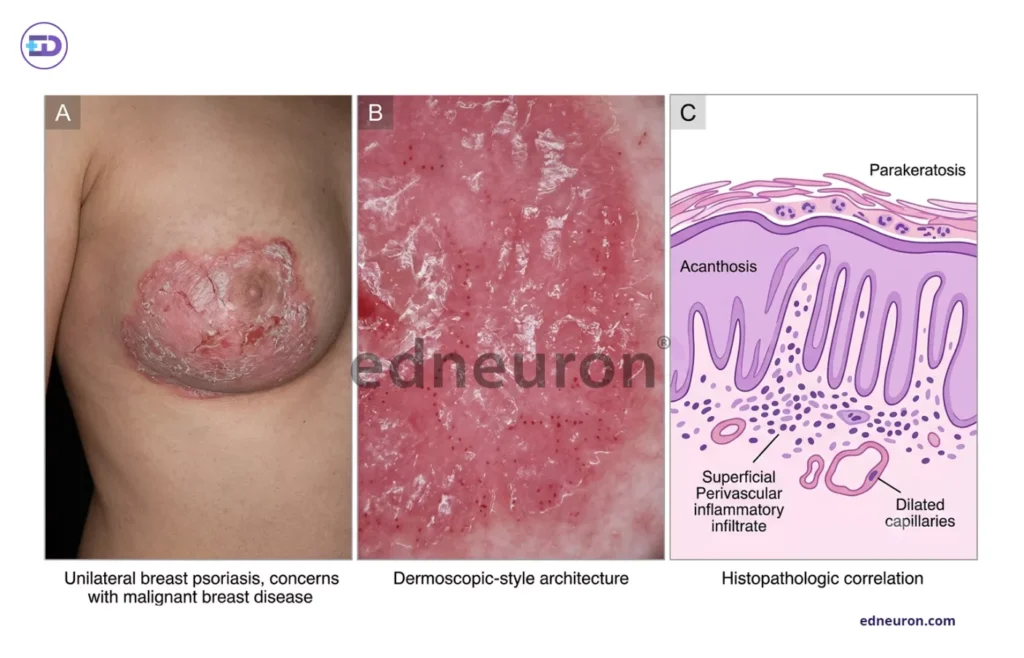
Fig 1: Clinicopathologic correlation of unilateral psoriatic plaque involving the breast region mimicking malignant inflammatory dermatosis.
A biopsy finally revealed the diagnosis. Samples from the nipple and the upper outer breast showed parakeratosis, thickened dermal layers, and enlarged dermal blood vessels. Tests for Cytokeratin-7 and E-cadherin were negative, ruling out Paget’s disease and other cancers.
Clinical Analysis
What makes this case notable is the profound diagnostic uncertainty created by the absence of systemic markers. In most presentations of psoriasis, the diagnosis is supported by the presence of characteristic silvery scales elsewhere on the body. In this patient, the isolated, unilateral nature of the plaque—combined with pain rather than pruritus—differed so sharply from the classic heuristic that psoriasis was initially excluded from the differential diagnosis.
One reason for the three-year delay was that doctors often look for cancer in older patients with changes in one breast. While this is important, it can lead them to miss inflammatory causes. Psoriasis on the nipple is rare and can sometimes be triggered by injury or the Koebner phenomenon, but no trigger was found here, making diagnosis even harder.
The diagnosis became clear after combining tissue analysis with targeted immune tests. Finding neutrophils in the scale crust and lymphocytes around blood vessels pointed to inflammation as the main cause. This led to a change from broad antimicrobials to a specific biologic treatment. The patient started Risankizumab, an IL-23 p19 inhibitor, and all symptoms and lesions disappeared within a month, confirming the disease was immune-related.
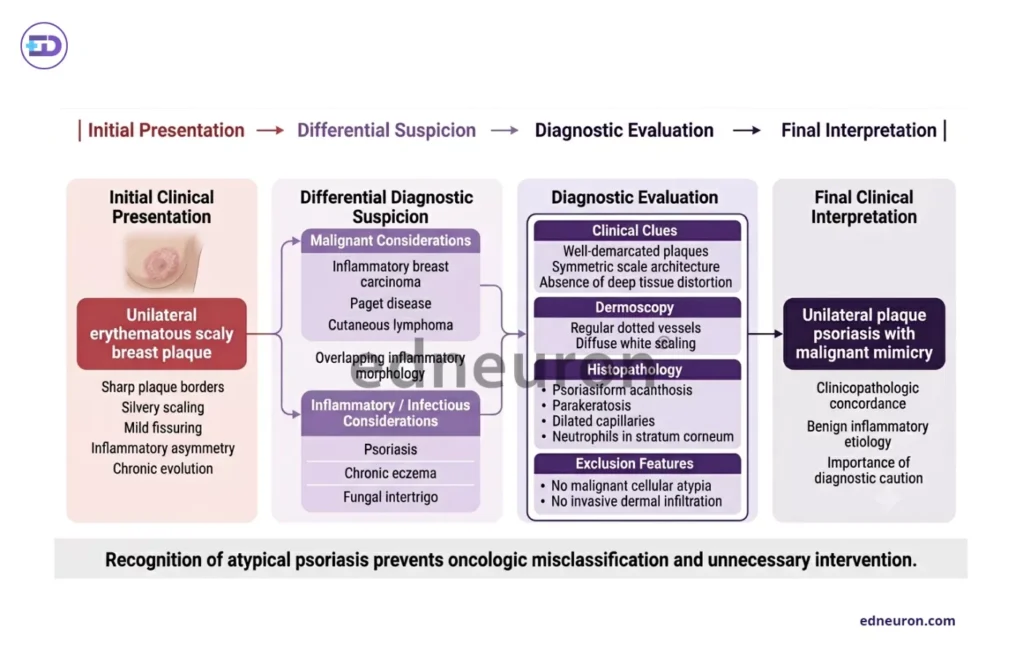
Fig 2 : Structured clinical evaluation differentiating unilateral breast psoriasis from malignant inflammatory breast disease mimics.
Clinical Implications
This case shows that where a lesion appears should not rule out a diagnosis if the appearance matches. Although the breast is a common site for cancer, it can also be affected by immune conditions like psoriasis. Doctors should look for the typical ‘micaceous scale’ even in unusual places.
This case also highlights the growing role of biologic drugs in treating stubborn, localized disease. Creams are usually tried first, but some areas are hard to treat this way and patients may not continue using them. For this patient, an IL-23 inhibitor that works throughout the body finally resolved her long-term symptoms.
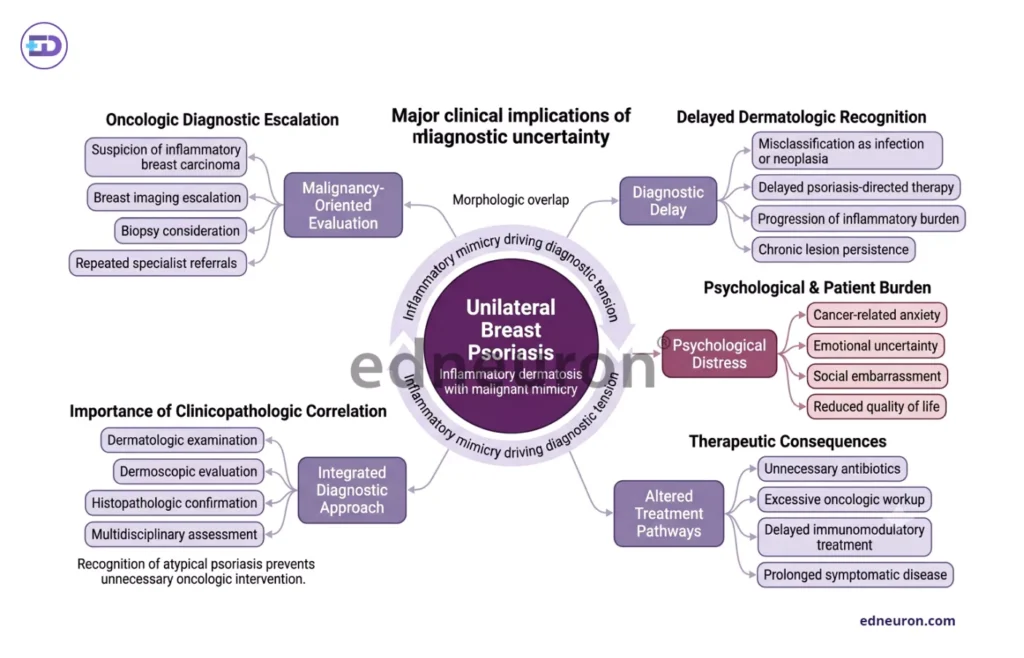
Fig 1 : Clinical implications arising from malignant mimicry in unilateral breast psoriasis and the importance of integrated diagnostic evaluation.
Conclusion
This case shows that while it is important to check for cancer in single breast plaques, doctors should also consider inflammatory causes. Psoriasis can look like cancer even without other signs, so the lesion’s appearance should guide the diagnosis.
- Key Clinical Takeaway: Solitary, painful breast lesions should be biopsied early to distinguish between cancer-like conditions and chronic inflammation.
- Management Implication: Biologic agents like risankizumab offer rapid resolution of recalcitrant, localized disease when traditional topicals fail due to anatomical or inflammatory factors.
References
- Mokni S, Ameur KB, Ghariani N, Denguezli M, Belajouza C, Nouira R, et al. A case of nail psoriasis successfully treated with intralesional methotrexate. Dermatol Ther (Heidelb). 2018 Dec;8(4):647-651. doi:10.1007/s13555-018-0261-2. PMID: 30232781. PMCID: PMC6232699.
- Relhan V, Sinha S, Khurana N, Garg VK. Multiple keratoacanthomas developing in healing plaques of psoriasis. Indian Dermatol Online J. 2013 Jul;4(3):202-204. doi:10.4103/2229-5178.115531. PMID: 24082182. PMCID: PMC3752476.
- Adjei S, Taha MR, Patel AB, Farah RS. Atypical presentation of psoriasis on the breast of an elderly woman: a case report. SAGE Open Med Case Rep. 2024;12:2050313X241292148. doi:10.1177/2050313X241292148. PMID: 39524494. PMCID: PMC11585343.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India