Introduction
For years, doctors have distinguished psoriasis from pityriasis rubra pilaris (PRP) by looking for features such as silvery scales, follicular papules, and ‘islands of sparing.’ But with the discovery of CARD14-associated papulosquamous eruption (CAPE), this way of thinking has changed. Now, we see that these conditions are actually different points along the same genetic spectrum. The main challenge for clinicians is not just identifying the skin lesion, but knowing when a patient’s poor response to standard treatments points to an underlying genetic cause.
The Molecular Convergence and Morphological Divergence
CAPE is caused by an activating mutation in the CARD14 gene. This gene makes a protein that helps control NF-κB signaling in the skin. Instead of a basic inflammatory response, this mutation leads to an overactive process in which NF-κB recruits additional inflammatory cells and increases the production of IL-23, IL-17, and IL-22.
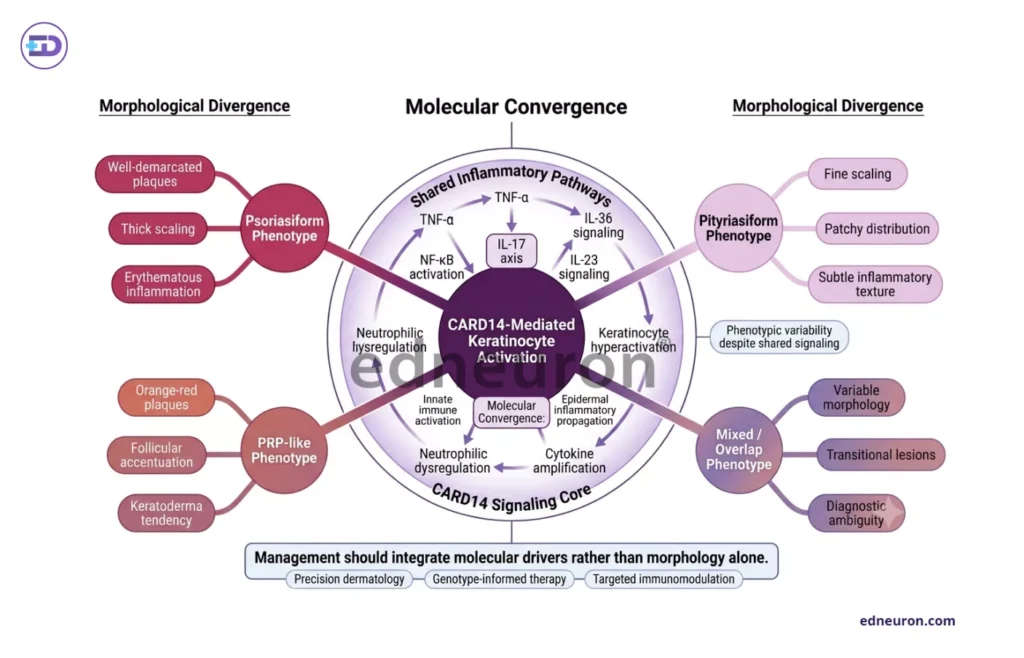
Fig 1 : Shared CARD14-driven inflammatory signaling produces heterogeneous papulosquamous phenotypes despite common molecular pathway activation.
This means that the different symptoms seen in these patients, from small red patches on the face to widespread skin redness, all come from the same underlying cause. Some families show a perfect match between the gene mutation and the symptoms, but others do not. This suggests that other factors, such as environmental factors or additional genes, may be required for the CARD14 mutation to cause disease. Because of this, the same mutation can look like ‘atypical juvenile PRP’ in one person and ‘extensive plaque psoriasis’ in another.
The Therapeutic Recalcitrance Dilemma
The biggest challenge in treating CAPE is that standard treatments for papulosquamous diseases usually do not work. While psoriasis and PRP often improve with topical steroids, phototherapy, or methotrexate, CAPE tends to resist these therapies, leaving patients and families frustrated. To make things harder, TNF-α inhibitors, which are often tried next, usually do not help when CARD14 is involved.
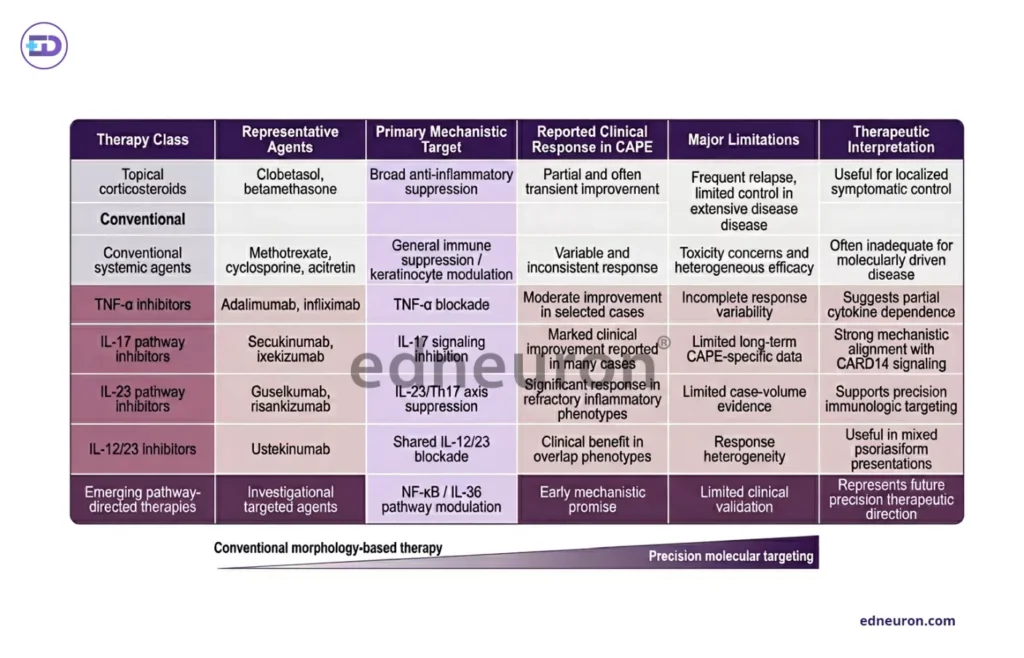
Table 1 : Comparative therapeutic response patterns in CAPE, highlighting the transition from conventional immunosuppression toward precision biologic targeting.
Studies show that moving from treatments based on appearance to those based on the disease mechanism makes a big difference. Since the CARD14 mutation activates the IL-23/Th17 pathway, drugs like ustekinumab, which block IL-12/23, have worked well when other treatments have not. Still, even these targeted drugs need careful use. Children with CAPE often need higher doses or more frequent treatments, such as every 8 weeks instead of 12, to keep the disease under control. This is especially true for patients who weigh more, as seen in adults with plaque psoriasis.
Real-World Implications and Diagnostic Red Flags
The translation of this evidence into clinical practice suggests a need for “precision dermatology” in the pediatric age group. A 12-month-old presenting with refractory “diaper dermatitis” that evolves into symmetric facial plaques should not merely be treated with more potent steroids; they should be evaluated for CAPE.
Key clinical indicators suggesting CAPE include:
- Early age of onset: Often appearing before one year of age.
- Characteristic facial distribution: Geometric pink-red patches on the cheeks, chin, and ears with sparing of the infralabial region.
- Atypical hybrid features: Overlap of psoriasis-like plaques and PRP-like “islands of sparing”.
- Family history: A strong autosomal dominant inheritance pattern of psoriasis or PRP.
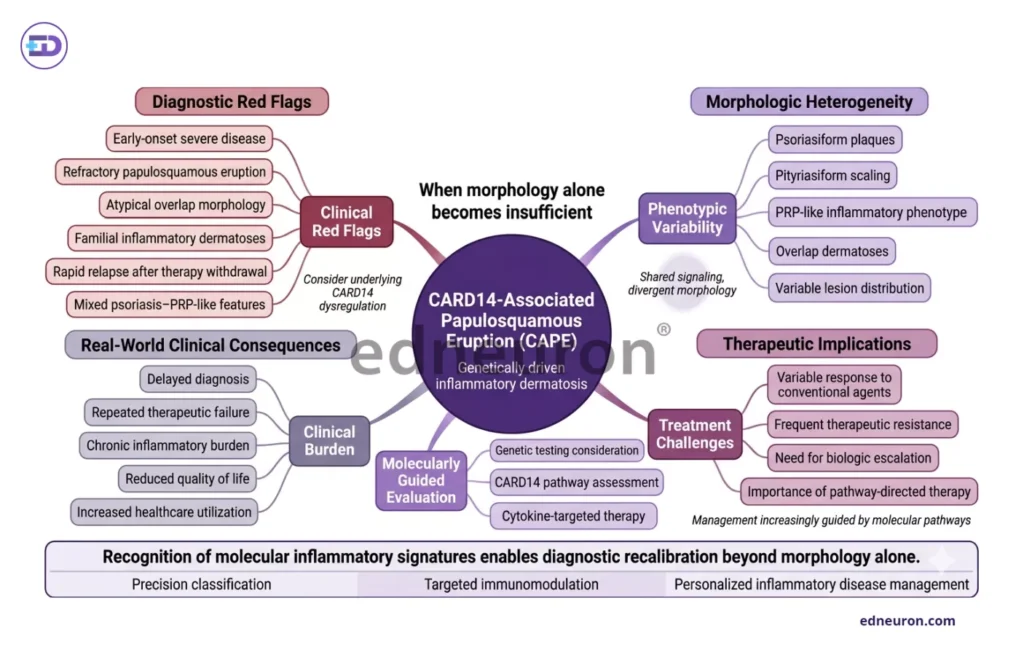
Fig 2 : Clinical red flags and real-world implications supporting molecularly informed diagnostic recalibration in CARD14-associated papulosquamous eruption.
Conclusion
CAPE represents a fundamental shift in our understanding of inflammatory skin disease. It teaches us that when anatomy and morphology provide an ambiguous verdict, the biological mechanism must guide the hand.
- Clinicians must lower the threshold for genetic testing in infancy-onset, refractory papulosquamous eruptions.
- The therapeutic goal should bypass broad immunosuppression in favor of precise IL-12/23 or IL-17 inhibition.
- Successful management requires a longitudinal commitment to dose optimization, acknowledging that “standard” regimens may be insufficient for this monogenic spectrum.
Ultimately, the most accurate diagnosis is the one that correlates with the molecular driver, allowing the clinician to move beyond “uncertainty management” and toward durable, life-altering clearance for these children.
References
- Jordan CT, Cao L, Roberson EDO, Duan S, Helms CA, Nair RP, et al. Rare and common variants in CARD14, encoding an epidermal regulator of NF-κB, in psoriasis. Am J Hum Genet. 2012;90(5):796-808. doi:10.1016/j.ajhg.2012.03.013. PMID: 22521419. PMCID: PMC3370271.
- Vaughan Jones SA, Hern S, Nelson-Piercy C, Seed PT, Black MM. A prospective study of 200 women with dermatoses of pregnancy correlating clinical findings with hormonal and immunopathological profiles. Br J Dermatol. 1999;141(1):71-81. doi:10.1046/j.1365-2133.1999.02939.x. PMID: 10417519.
- Errichetti E, Stinco G. Dermoscopy in general dermatology: a practical overview. Dermatol Ther (Heidelb). 2016;6(4):471-507. doi:10.1007/s13555-016-0141-6. PMID: 27613297. PMCID: PMC5096246.
- Grace D, Kumar S, Valand AG, et al. Spectrum of non-infectious erythematous, papular and squamous lesions of the skin: a histopathological study. Indian J Dermatol. 2010;55(3):225-228. doi:10.4103/0019-5154.70669. PMID: 20952839. PMCID: PMC2965905.
- Raghuveer CV, Mahajan VK, Mehta KS, Chauhan PS, Sharma V. Clinico-histopathological correlation of papulosquamous disorders: a retrospective study. Int J Res Med Sci. 2018;6(3):1048-1054. doi:10.18203/2320-6012.ijrms20180845.
- Jain VK, Jindal N, Imchen S, et al. Clinical pattern of papulosquamous dermatoses: an observational study conducted at a tertiary care center, Ujjain. Int J Res Dermatol. 2018;4(2):220-224. doi:10.18203/issn.2455-4529.IntJResDermatol20180989.
- Dogra S, Kaur I, Kumar B. Pattern of papulosquamous disorders in children: a clinico-epidemiological study. Pediatr Dermatol. 2022;39(2):256-262. doi:10.1111/pde.14875. PMID: 35186517.
- Craiglow BG, Boyden LM, Hu R, Virtanen M, Su J, Rodriguez G, et al. CARD14-associated papulosquamous eruption (CAPE) in pediatric patients: three additional cases and review of the literature. Pediatr Dermatol. 2021;38(6):1387-1393. doi:10.1111/pde.14776. PMID: 34448248. PMCID: PMC8512413.
- Theodoridis A, Gkrouzman E, Kassamali B, et al. Clinical and laboratory prognosticators of atrophic papulosis (Degos disease): a systematic review. J Am Acad Dermatol. 2021;85(5):1287-1295. doi:10.1016/j.jaad.2021.03.045. PMID: 33957947.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India