
Introduction
Traditionally, strabismus treatment has focused on achieving a straight-looking eye as the main sign of surgical success. Yet, for many clinician-scientists, this cosmetic result can hide more serious problems with sensory integration. We often see patients who had straight eyes as children but return years later with symptoms that cannot be fixed by glasses alone. These cases make us question the idea of a strict ‘critical period’ and ask when cosmetic alignment might actually cause problems for patients.
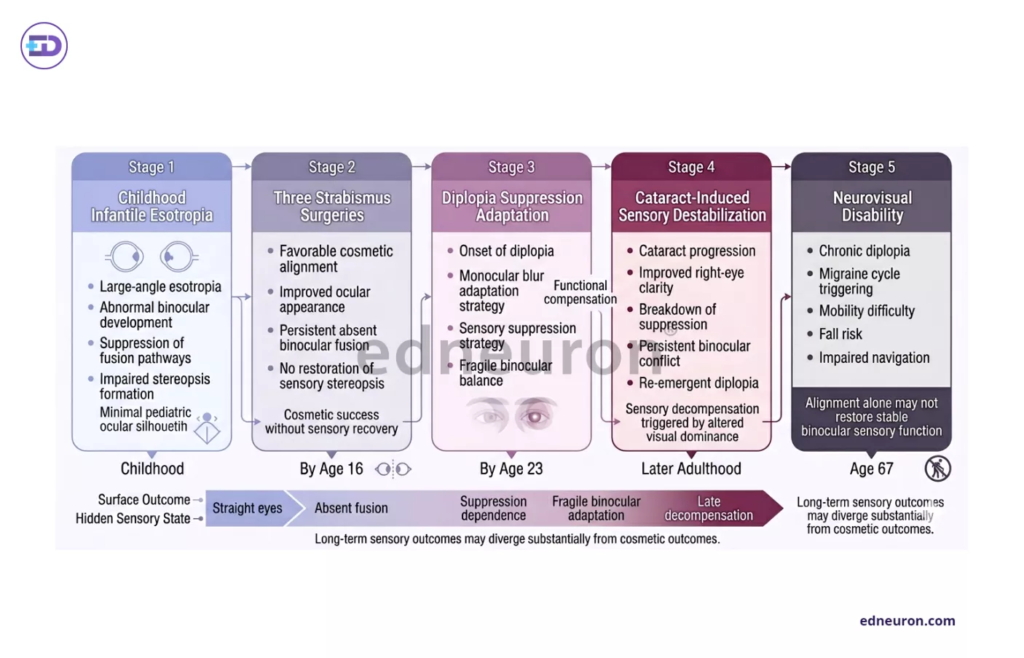
Fig 1 : Longstanding sensory suppression after cosmetically successful childhood strabismus correction may later decompensate, producing disabling diplopia and neurovisual dysfunction.
Case Presentation
A 67-year-old female presented with a complex, 14-year history of increasing double vision and complete migraine cycles triggered by the onset of diplopia. Her medical history was a chronicle of the historical standard of care: three strabismus surgeries by age 16 for infantile esotropia. While these interventions achieved “favorable cosmesis,” they failed to address sensory perception or binocular fusion.
By age 23, she developed clear double vision, which she managed by intentionally blurring one eye to ignore the second image. This delicate balance was lost when she developed cataracts with age. As her right eye started to see better than her dominant left, she could no longer block out the second image. This led to trouble moving around and caused her to fall recently.
Clinical Analysis / Discussion
What makes this case notable is the divergence between motor alignment and sensory stability. In this patient, the eyes appeared cosmetically straight, yet she suffered from a 12D constant right esotropia with a 1D vertical component. This highlights a critical tension in strabismus management: the historical reliance on surgery alone often ignores the neuro-visual pathways necessary for binocularity.
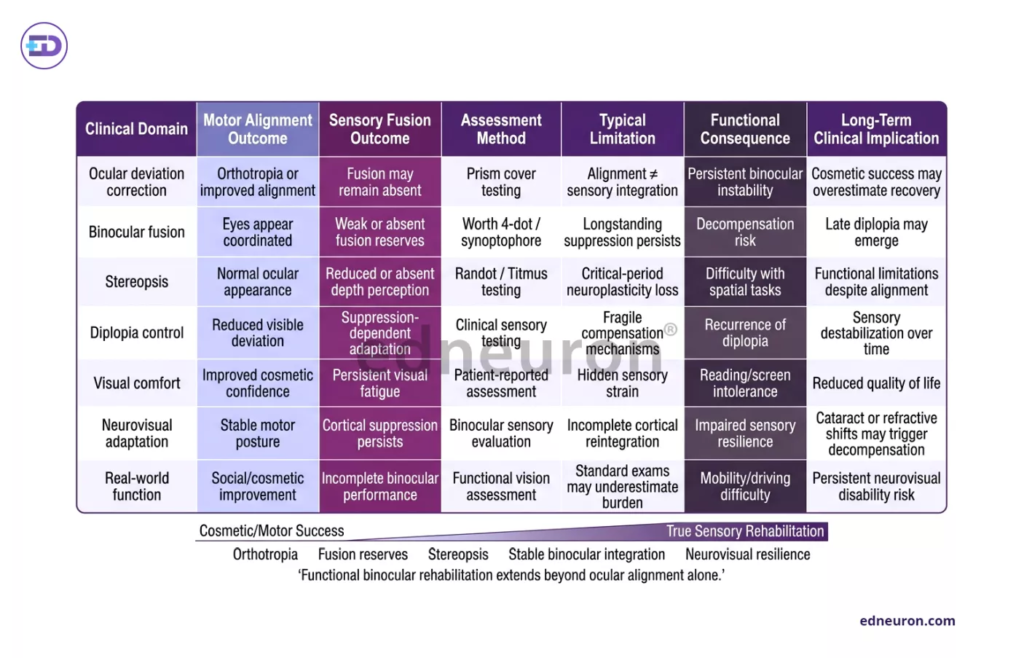
Table 1 : Motor alignment after strabismus treatment may not correlate with restoration of stable binocular sensory fusion or long-term neurovisual function.
One likely reason for her problems later in life is that repeated surgeries disrupted the feedback from her eye muscles, especially since she never developed strong brain-eye connections through vision therapy. Recent studies show that surgery can interfere with this feedback, making it harder to recover if binocular vision was never built up. While it was once thought that adults could not benefit from sensory retraining because of ‘critical periods,’ new research on neuroplasticity shows that vision therapy can help people of any age by improving eye coordination and reducing suppression.
The complexity of this sensory-motor interaction is echoed in other forms of acquired strabismus. For instance, in Acute Acquired Comitant Esotropia (AACE), excessive near work (such as smartphone use) can induce a dynamic preponderance of the medial rectus muscles, even in patients with previously good binocularity. Similarly, cases of cyclic vertical deviation demonstrate that the brain’s internal “biological clock” can trigger or resolve strabismic phases in response to underlying systemic conditions such as dysthyroid ophthalmopathy.
These different cases show one main idea: eye alignment is not fixed but always changing. In our 67-year-old patient, the new problem of a cataract was enough to upset the balance she had maintained for many years.
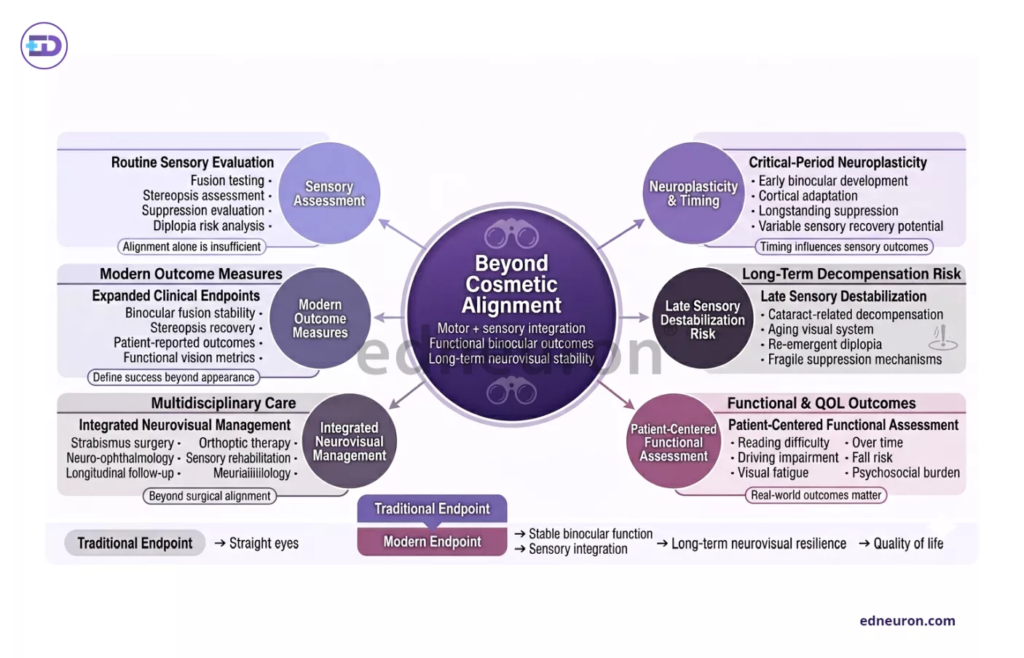
Fig 2: Comprehensive strabismus management requires integration of cosmetic alignment, sensory fusion, neurovisual function, and patient-centered quality-of-life outcomes.
Clinical Implications
This case teaches us that cosmetic surgery is not a surrogate for a cure. When we treat the motor deviation without addressing the sensory gap, we leave the patient vulnerable to “sensory failure” later in life, when their compensatory mechanisms (such as suppression or head tilting) inevitably fail.
Real-world practice must shift toward a collaborative, sequential model. As illustrated in contemporary treatment algorithms, vision therapy should ideally be initiated prior to surgery to establish the neuro-visual foundation for fusion. If surgery is required, it must be followed by further therapy to ensure the integration of sensory and motor fusion.
Conclusions
A ‘straight eye’ that looks normal does not always mean the patient is healthy. As clinicians, we need to look past test results and focus on how the patient actually sees and experiences the world.
- Sensory Integration is Paramount: Long-term success requires addressing visual sensory perception, not just muscle repositioning.
- The Myth of the Critical Period: Neuroplasticity allows for functional improvements well into adulthood; age should not be a barrier to vision therapy.
- Working together across specialties leads to the best results. The best care involves a series of steps: optical correction, vision therapy, and surgery if needed when progress stalls.
- Anticipate Lifecycle Changes: Patients with a history of strabismus surgery require vigilant monitoring during later life transitions, such as cataract development, which can destabilize fragile sensory compensation.
References
- Lee HS, Park SW, Heo H. Acute acquired comitant esotropia related to excessive Smartphone use. BMC Ophthalmol. 2016;16:37. doi:10.1186/s12886-016-0213-5. PMID: 27063647. PMCID: PMC4826517.
- Yuan Y, Wang X, Ling L, Yu X, Jiang C, Wen W, et al. Unexpected extraocular muscle hypoplasia during strabismus surgery: case series. BMC Ophthalmol. 2024;24(1):517. doi:10.1186/s12886-024-03787-x. PMID: 39623321. PMCID: PMC11610363.
- Kim DH, Kim H, Choi DG. A cyclic vertical deviation with dysthyroid ophthalmopathy: a case report. BMC Ophthalmol. 2016;16:139. doi:10.1186/s12886-016-0300-7. PMID: 27553295. PMCID: PMC4990895.
- Chatzistefanou KI, Droutsas KD, Chimonidou E, Moschos MM. Adult-onset acute concomitant esotropia: clinical characteristics and management. Clin Ophthalmol. 2009;3:307-311. doi:10.2147/OPTH.S5133. PMID: 19668580. PMCID: PMC2728021.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



