
Introduction
Optic neuritis (ON) is often seen as a success in neuro-ophthalmology, with patients typically regaining functional vision quickly. Still, relying mainly on high-contrast visual acuity has led to an underestimation of ongoing nerve damage. Recent long-term studies show that recovery is more complex, as the visual system can hide lasting structural damage by using its built-in redundancy and ability to adapt.
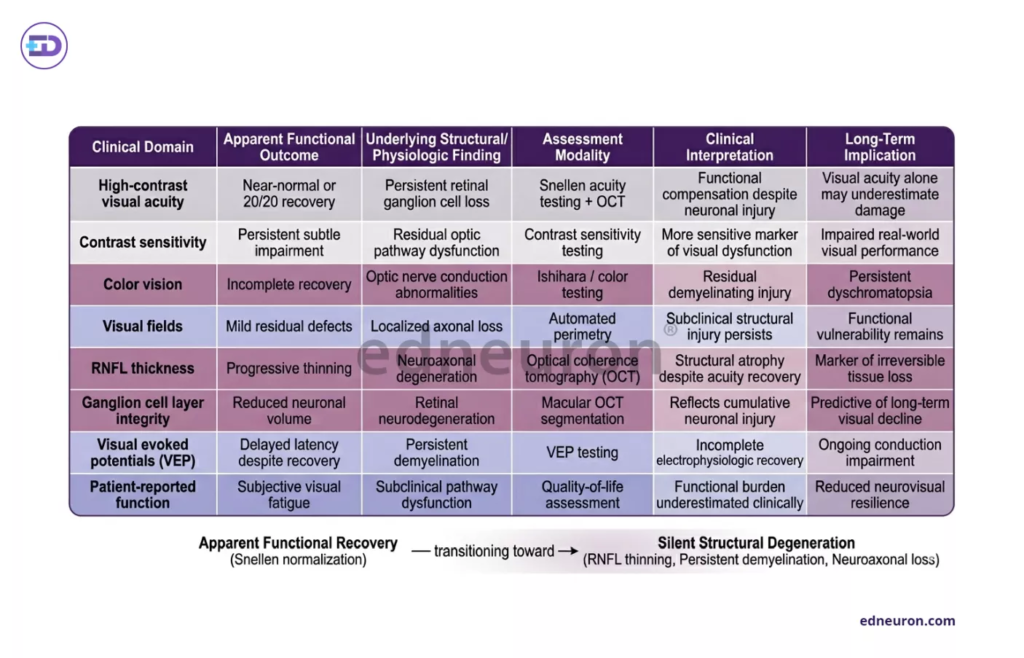
Table 1 : Apparent visual recovery after acute optic neuritis may mask persistent neuroaxonal degeneration detectable through structural and neurophysiologic assessment.
The Mirage of the 20/20 Outcome
The Optic Neuritis Treatment Trial (ONTT) showed that more than 90% of patients regain visual acuity of 20/40 or better. However, the Snellen chart does not reflect the full patient experience. Even when high-contrast vision returns to normal, low-contrast letter acuity (LCLA) often shows lasting problems. This means the visual system tends to preserve sharp vision but loses the subtle sensitivity needed for tasks like reading in low light or recognizing faces.
Another challenge is the gap between how well the eye works and its actual structure. Optical Coherence Tomography (OCT) often shows thinning of the peripapillary retinal nerve fiber layer (pRNFL) and the macular ganglion cell-inner plexiform layer (mGCIPL), even in eyes with 20/20 vision. This thinning means there is real loss of nerve fibers and cells. It raises an important question: when does the visual system’s backup capacity run out, causing permanent disability after more attacks?
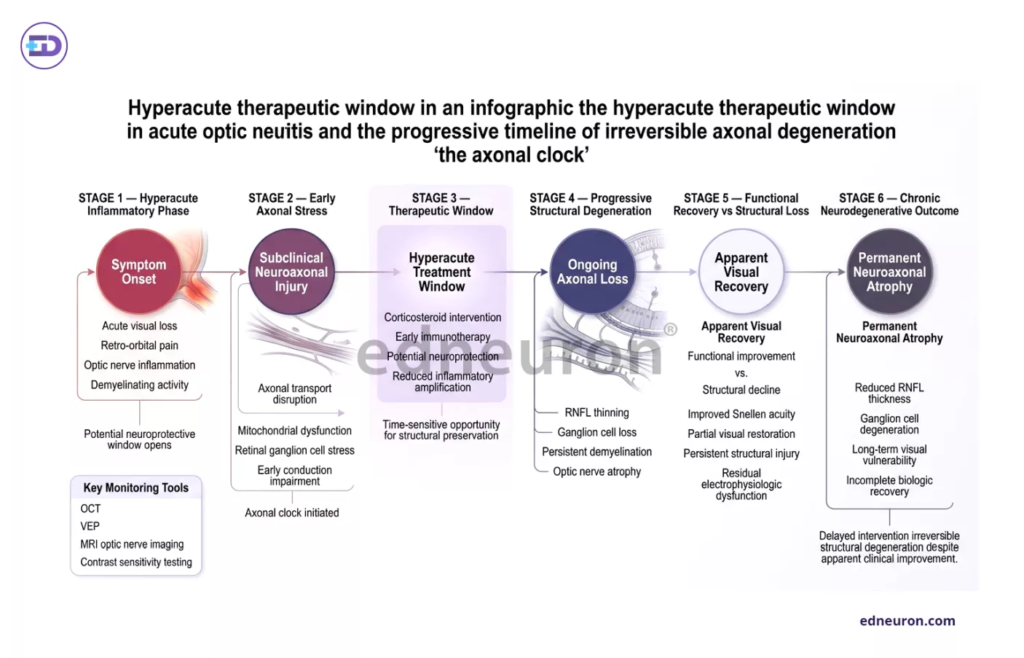
Fig 1 : Time-dependent neuroaxonal degeneration in acute optic neuritis highlights a limited hyperacute therapeutic window despite apparent functional visual recovery.
The Hyperacute Window and the Axonal Clock
The disease process in ON progresses rapidly. Inflammation first blocks nerve signals, but permanent damage to nerve fibers can take place within five to seven days. This creates a key question about when to use corticosteroids. The ONTT found that steroids speed up recovery but do not change long-term results; the trial did not assess “hyperacute” intervention—defined as treatment within 48 hours of symptom onset.
One likely reason standard treatments do not stop nerve loss is that, by the time therapy begins, nerve damage has already started. New research shows that treatment needs to happen before severe myelin loss and nerve damage occur. The differences between ON types also make things more complicated. In multiple sclerosis (MS)-related ON, the outlook is usually good. But in neuromyelitis optica spectrum disorder (NMOSD) or myelin oligodendrocyte glycoprotein (MOG)-IgG disease, the first attack is often much more damaging, and steroids alone do not prevent blindness in up to 30% of cases.
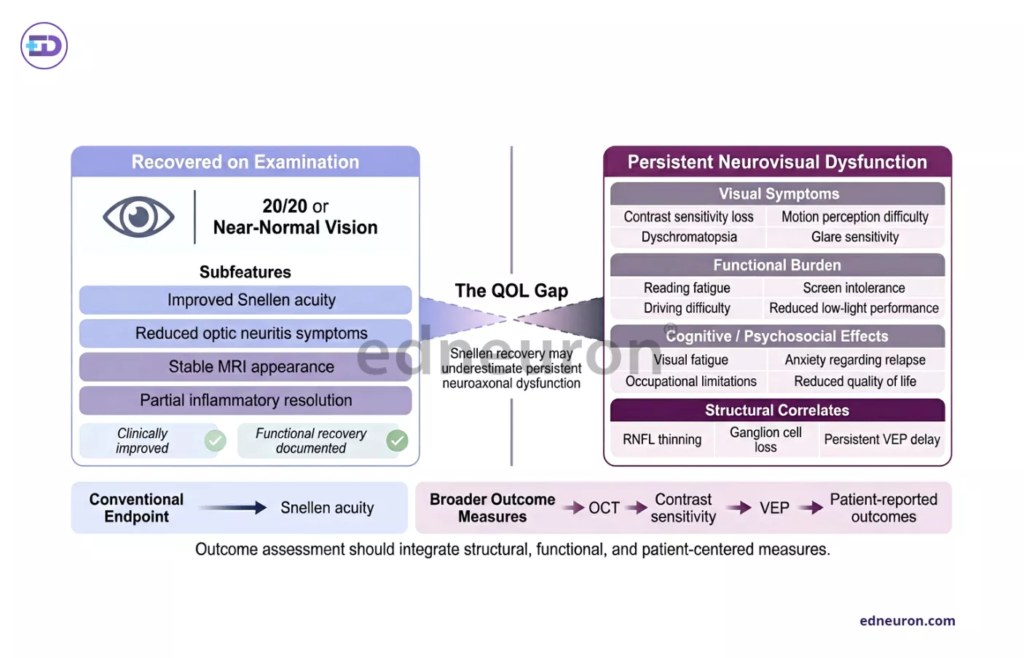
Fig 2: Near-normal visual acuity after optic neuritis may mask persistent neuroaxonal injury and substantial real-world quality-of-life impairment.
Real-World Implications and the QOL Gap
We need to redefine ‘recovery’ in clinical practice to include quality-of-life (QOL) measures. Many patients still have trouble with motion perception (Pulfrich’s phenomenon) and vision that blurs with temperature changes (Uhthoff’s symptom), which standard scales often miss. In the UK, where many ON cases are not clearly defined, it is important to spot ‘atypical’ cases early. Signs such as both eyes being affected, no pain, or very severe vision loss (no light perception) are warning signs that warrant strong immunosuppression and possibly plasma exchange (PLEX) to prevent permanent damage.
Conclusions
When diagnosing acute optic neuritis, we should move from just checking visual acuity at one point in time to regularly assessing nerve health over time.
- To better measure success, clinicians should look beyond Snellen acuity and focus on LCLA and OCT findings of ganglion cell loss as main signs of disease impact.
- The ‘Time is Vision’ approach means starting treatment, especially for repeat or unusual cases, within 48 hours to give the best chance of protecting nerve structure.
- Atypical Vigilance: Early identification of NMOSD and MOG-IgG phenotypes is essential, as these conditions require a fundamentally different management strategy involving PLEX and long-term steroid-sparing agents.
Ultimately, the goal of management is no longer just to speed the resolution of an attack, but to defend the integrity of the optic nerve against a silent, cumulative decay.
References
- Phuljhele S, Kedar S, Saxena R. Approach to optic neuritis: An update. Indian J Ophthalmol. 2021 Sep;69(9):2266-2276. doi:10.4103/ijo.IJO_3415_20. PMID: 34427197. PMCID: PMC8544067.
- Bennett JL. Optic neuritis. Continuum (Minneap Minn). 2019 Oct;25(5):1236-1264. doi:10.1212/CON.0000000000000768. PMID: 31584536. PMCID: PMC7395663.
- Menon V, Saxena R, Misra R, Phuljhele S. Management of optic neuritis. Indian J Ophthalmol. 2011 Mar-Apr;59(2):117-122. doi:10.4103/0301-4738.77015. PMID: 21350266. PMCID: PMC3116540.
- Kale N. New developments in the treatment of optic neuritis. Eye Brain. 2010 Sep 15;2:49-59. doi:10.2147/EB.S6871. PMID: 23225902. PMCID: PMC5436165.
- Petrillo LA, Balcer LJ, Galetta SL. Acute optic neuritis: Unmet clinical needs and model for new therapies. Drug Discov Today. 2015 Jan;20(1):78-84. doi:10.1016/j.drudis.2014.09.010. PMID: 25284754. PMCID: PMC4516397.
- Chen JJ, Bhatti MT. Disease course of clinically isolated optic neuritis. Neurol Neuroimmunol Neuroinflamm. 2024;11(2):e200223. doi:10.1212/NXI.0000000000200223. PMID: 38346762. PMCID: PMC10856731.
- Bennett JL, de Seze J, Lana-Peixoto M, Palace J, Waldman A, Schippling S, et al. The changing landscape of optic neuritis: A narrative review. J Neuroophthalmol. 2021 Sep;41(3):e519-e532. doi:10.1097/WNO.0000000000001187. PMID: 33560705. PMCID: PMC8253868.
- Ambika S, Lakshmi P. How far should I manage acute optic neuritis as an ophthalmologist? A United Kingdom perspective. Eye (Lond). 2024 Aug;38(12):2285-2293. doi:10.1038/s41433-024-03164-4. PMID: 38849321.
- Abdelhak A, Elsone L, Tuleasca C, Kuhle J, Krbot Skoric M, Martin R, et al. The effect of Optic Neuritis Treatment Trial combined corticosteroid regimen on pattern reversal visual evoked potentials. BMC Ophthalmol. 2021 Aug 18;21(1):320. doi:10.1186/s12886-021-02086-z. PMID: 34407772. PMCID: PMC8374875.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



