

Introduction
Cataract remains the main cause of reversible blindness around the world, and the problem is getting worse as people live longer and fewer specialists are available. Artificial intelligence (AI) can help achieve faster diagnoses and more accurate results, but its performance in clinical settings is less consistent than in controlled studies. This puts clinicians in a tough spot, as they have to balance the advantages of AI with concerns about its real-world reliability and the clarity of its decisions.
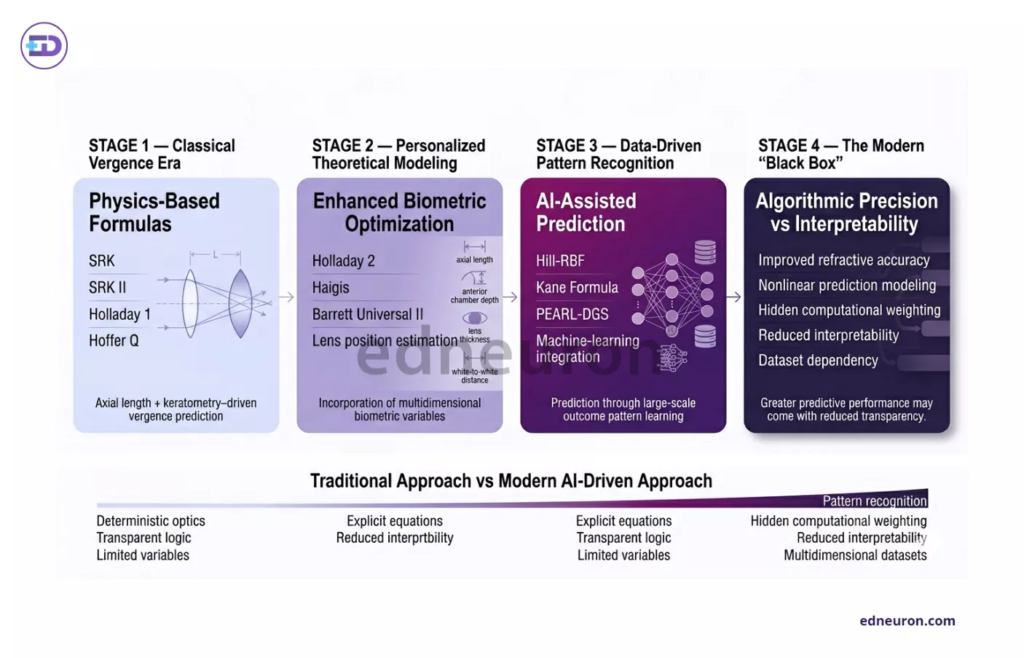
Fig 1 : Modern IOL calculation has evolved from transparent, physics-based formulas to increasingly accurate yet less interpretable AI-driven predictive systems.
The Predictive Shift: From Physics to Patterns in IOL Calculation
Doctors have long relied on linear vergence formulas to select the appropriate power for intraocular lenses (IOLs), but these methods often fall short in eyes with unusual measurements. AI-based formulas like Kane and Hill-Radial Basis Function (RBF) use pattern recognition and advanced computing to make better predictions. For patients with very short or very long axial lengths (≤22.0mm or ≥26.0mm), these AI tools have produced much lower average errors than older formulas like Haigis or Hoffer Q.
However, this precision introduces a new clinical variable: the “black box” effect. Because the specific algorithm details for formulas like the Kane remain proprietary or mathematically opaque, the clinician must decide whether to trust a superior numerical prediction without understanding the underlying logic. It suggests that while AI may minimize “refractive surprises,” it also places the surgeon in an uncomfortable position by delegating a critical surgical decision to an uninterpretable model.
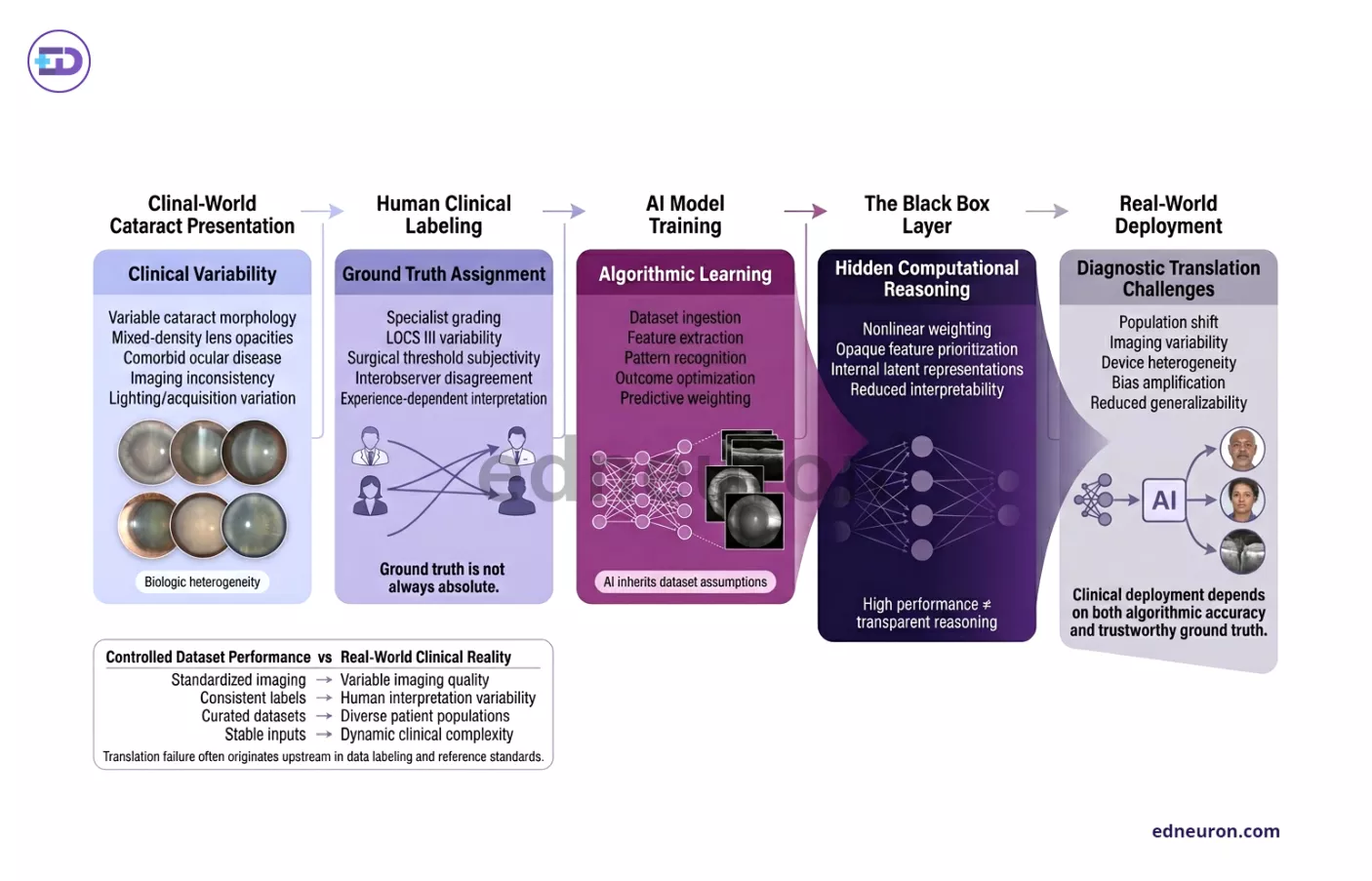
Fig 2 : AI performance in cataract diagnostics depends fundamentally on the reliability, consistency, and clinical validity of human-defined ground truth data.
Diagnostic Translation and the “Ground Truth” Dilemma
The deployment of deep learning (DL) for cataract screening using slit-lamp and color fundus photographs has produced staggering internal validation results, with some systems achieving area under the curve (AUC) metrics exceeding 0.99. This capability is particularly vital in low-resource settings where the shortage of trained ophthalmologists often leaves significant proportions of the population undiagnosed. By leveraging existing diabetic retinopathy screening infrastructure, AI can provide opportunistic cataract detection with minimal additional cost.
Another challenge is that the “ground truth” used to train these models is often subjective. Many algorithms rely on doctors’ ratings of “visibility” or “haziness,” which can vary from one examiner to another. If AI is trained on these personal judgments rather than clear anatomical standards, it may simply reproduce human biases. This means that current AI detection is only as good as the expertise of the doctors who labeled the data, showing the need for better, more consistent clinical datasets.
Real-World Outcomes and Surgical Coaching
Beyond the preoperative stage, AI is increasingly positioned as an intraoperative “coach.” Systems such as PhacoTracking and DeepPhase utilize convolutional neural networks to identify surgical phases and track instrument movements in real-time. These tools provide an objective metric for resident training, identifying non-optimal procedures before they lead to acute mechanical injuries such as posterior capsule rupture.
Postoperatively, AI models such as TempSeq-Net have demonstrated 92.2% accuracy in predicting the progression of posterior capsule opacification (PCO). This allows for a shift from reactive to proactive care, enabling clinicians to identify at-risk individuals and plan YAG laser capsulotomy interventions before visual function is significantly compromised.
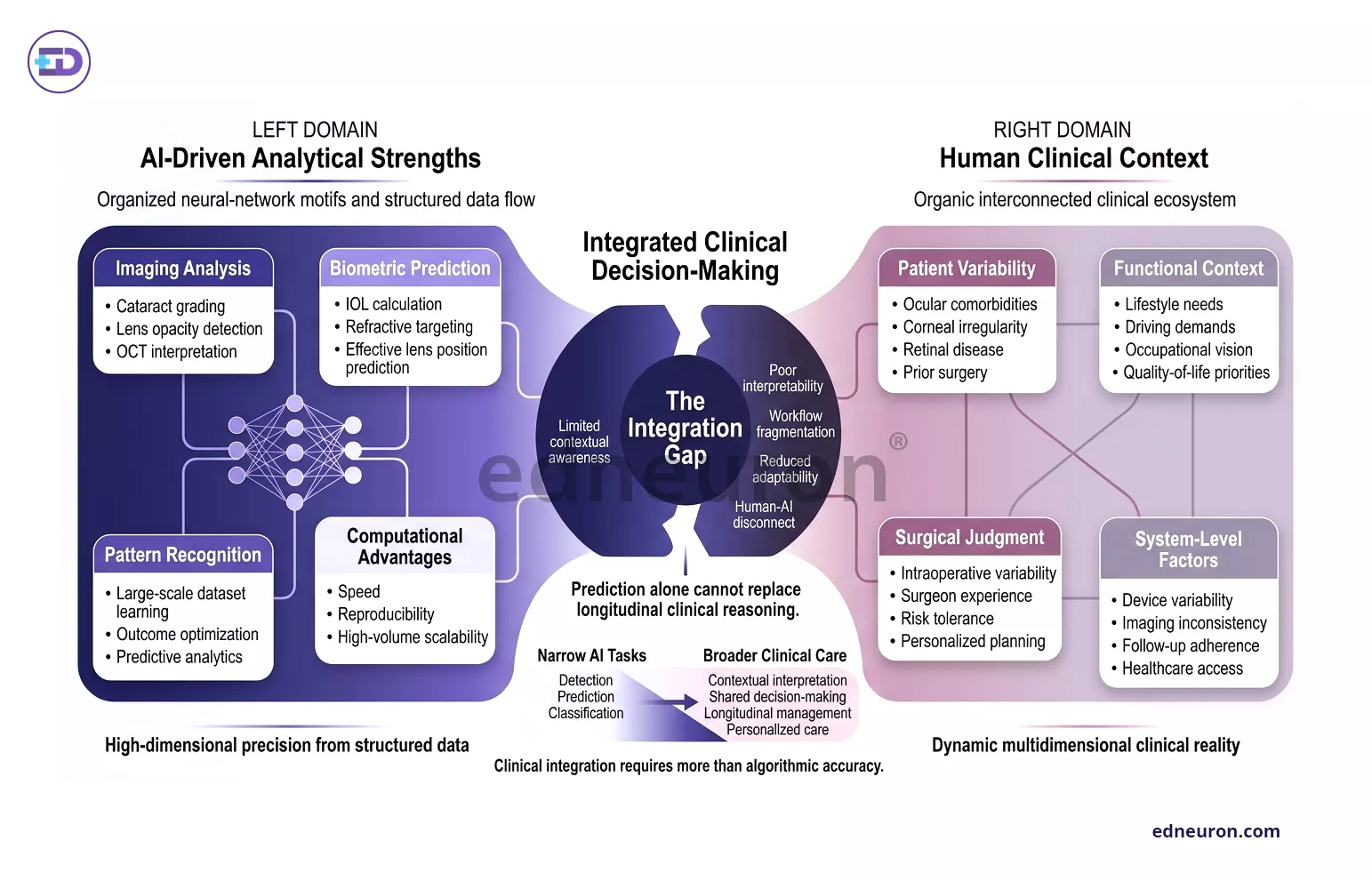
Fig 3: The clinical value of AI in cataract management depends not only on predictive accuracy, but also on successful integration into complex real-world ophthalmic decision-making.
Broader Perspective: The Integration Gap
The main goal is to move from strong algorithm results to real use in clinics. Platforms like “CC-guardian” and other remote diagnostic tools show how care can be distributed, but differences in surgical quality between rich and poorer countries remain a major challenge. For AI to reach its full potential, it needs to become more transparent and be tested with standard measures in diverse patient groups.
Conclusions
AI in cataract management is moving from an experimental curiosity to a fundamental refractive and diagnostic tool. To optimize this transition, clinicians should prioritize the following strategies:
- Targeted Formula Selection: Use AI-based formulas (Kane, Hill-RBF 3.0) specifically for biometric outliers where traditional vergence models are known to fail.
- Vigilant Oversight: Treat AI screening outputs as high-sensitivity triaging tools rather than definitive diagnoses, especially when “ground truth” data remains unstandardized.
- Data Security and Ethics: Advocate for federated learning and transparent reporting (CONSORT-AI) to ensure that the pursuit of precision does not compromise patient privacy.
References
- Mehta H, Tufail A, Da Cruz L, et al. Management of cataract in patients with age-related macular degeneration. J Clin Med. 2021;10(12):2538. doi:10.3390/jcm10122538. PMID: 34204385.
- Ting DSW, Pasquale LR, Peng L, et al. Artificial intelligence and deep learning in ophthalmology. Br J Ophthalmol. 2019;103(2):167-175. doi:10.1136/bjophthalmol-2018-313173. PMID: 30361318.
- Ahuja AS, Farford BA, Forouhi M, et al. Applications of artificial intelligence in cataract surgery: a review. Clin Ophthalmol. 2024;18:101-118. doi:10.2147/OPTH.S489054. PMID: 39412357.
- Ting DSW, Ang M, Mehta JS, Ting DSW. Application of artificial intelligence in cataract management: current and future directions. Eye Vis (Lond). 2021;8(1):3. doi:10.1186/s40662-021-00227-0. PMID: 35000627.
- Wang Y, Liu X, Chen H, et al. Lens capsule-related complications in cataract phacoemulsification. Adv Ophthalmol Pract Res. 2026;6(1):100052. doi:10.1016/j.aopr.2026.100052.
- Han X, Zhang Y, Wang W, et al. Real-world visual outcomes of cataract surgery based on population-based studies: a systematic review. Br J Ophthalmol. 2023;107(8):1041-1049. doi:10.1136/bjo-2022-321876. PMID: 36323491.
- Zhang JH, McGuinness MB, Keel S, et al. A systematic review of clinical practice guidelines for cataract. Vision (Basel). 2022;6(2):36. doi:10.3390/vision6020036. PMID: 35622547.
- Sachdev M. Cataract surgery: the journey thus far. Indian J Ophthalmol. 2017;65(12):1267-1268. doi:10.4103/ijo.IJO_1104_17. PMID: 29208808.
- Allen D. Cataract. BMJ Clin Evid. 2011;2011:0704. PMID: 21718567.
- Khamkar SG, Patil AV, More SS, et al. Review on cataract. Indian J Cataract Refract Surg. 2024;2(1):15-24. doi:10.4103/ijcrs.ijcrs_12_24.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



