

Introduction
Glaucoma is often called the “silent thief of sight” because early treatment can prevent it, yet nearly half of the cases in developed countries are not diagnosed until permanent damage has occurred. Optical Coherence Tomography (OCT) has made it easier to detect small changes in retinal ganglion cells (RGCs). Still, translating these detailed images into a clear diagnosis is challenging due to human error and the complexity of thickness maps. This shows there is a gap between the precision of our imaging tools and our ability to interpret them. Deep learning (DL) offers a way to bridge this gap, but it also introduces new challenges.
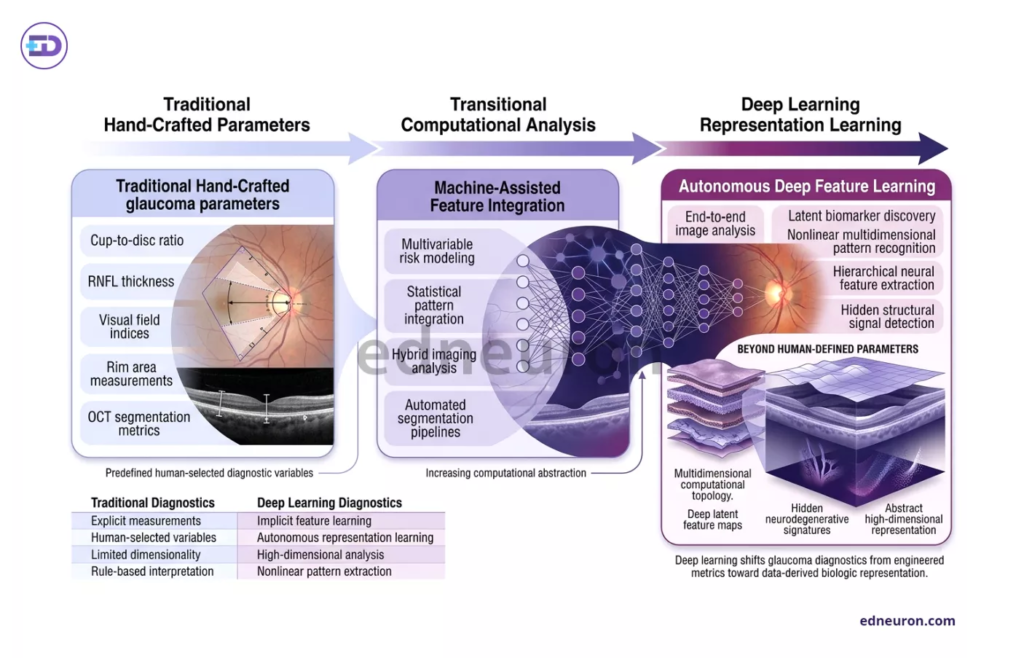
Fig 1 : Deep learning transforms glaucoma diagnostics by shifting from predefined human-engineered measurements toward autonomous multidimensional feature discovery directly from imaging data.
The Departure from Hand-Crafted Parameters
Traditionally, diagnosing glaucomatous optic neuropathy has depended on “hand-crafted” parameters, which are clinician-defined metrics like retinal nerve fiber layer (RNFL) thickness or Bruch’s membrane opening-minimum rim width (BMO-MRW). However, these metrics often face a “measurement floor,” where automated segmentation cannot detect further progression in moderate-to-advanced disease. Recent research points to a shift toward “segmentation-free” models that analyze raw volumetric data directly.
Studies show that Convolutional Neural Networks (CNNs) can extract layered information from OCT B-scans, thereby avoiding the errors associated with traditional layer-by-layer segmentation. For example, geometric deep learning solutions such as PointNet, which represent the optic nerve head as a 3D point cloud, have achieved diagnostic accuracy (AUC 0.95), significantly outperforming the current clinical gold standard of RNFL thickness alone (AUC 0.80). These results suggest that DL is powerful because it can detect subtle structural features, possibly in the lamina cribrosa or deep peripapillary sclera, that are difficult to discern manually.
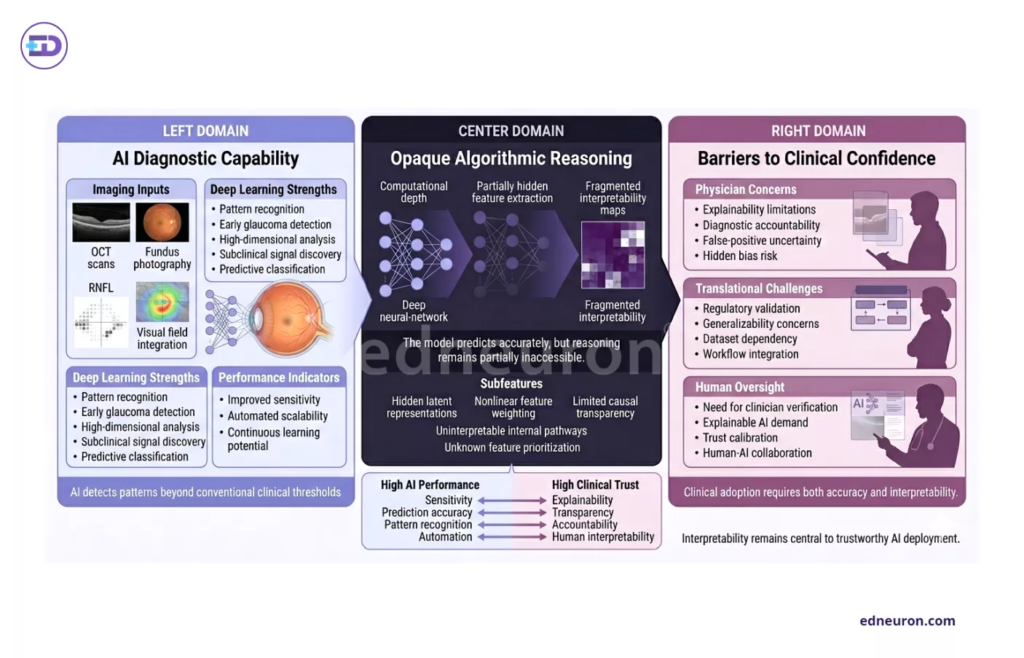
Fig 2 : Despite high diagnostic performance, deep learning systems in glaucoma care face persistent challenges in interpretability, accountability, and clinician trust.
The “Black Box” and the Burden of Clinical Trust
One challenge with this new technology is that DL works like a “black box,” making its complex processes hard for clinicians to understand. In medicine, where treatment decisions can mean lifelong medication or surgery, a diagnosis without a clear explanation creates an ethical problem. Because of this, using Explainable AI (XAI) is now a clinical necessity, not just a technical improvement.
Techniques like Class Activation Maps (CAM) and Grad-CAM aim to show how the model makes decisions by highlighting the specific anatomical regions, such as the superior or inferior neuroretinal rim, that the model considers most important. When these “heatmaps” match known clinical patterns of RGC loss, clinicians trust the results more. But if the model focuses on unexpected areas, such as the photoreceptor layers, it raises questions about whether they are new biomarkers or imaging artifacts.
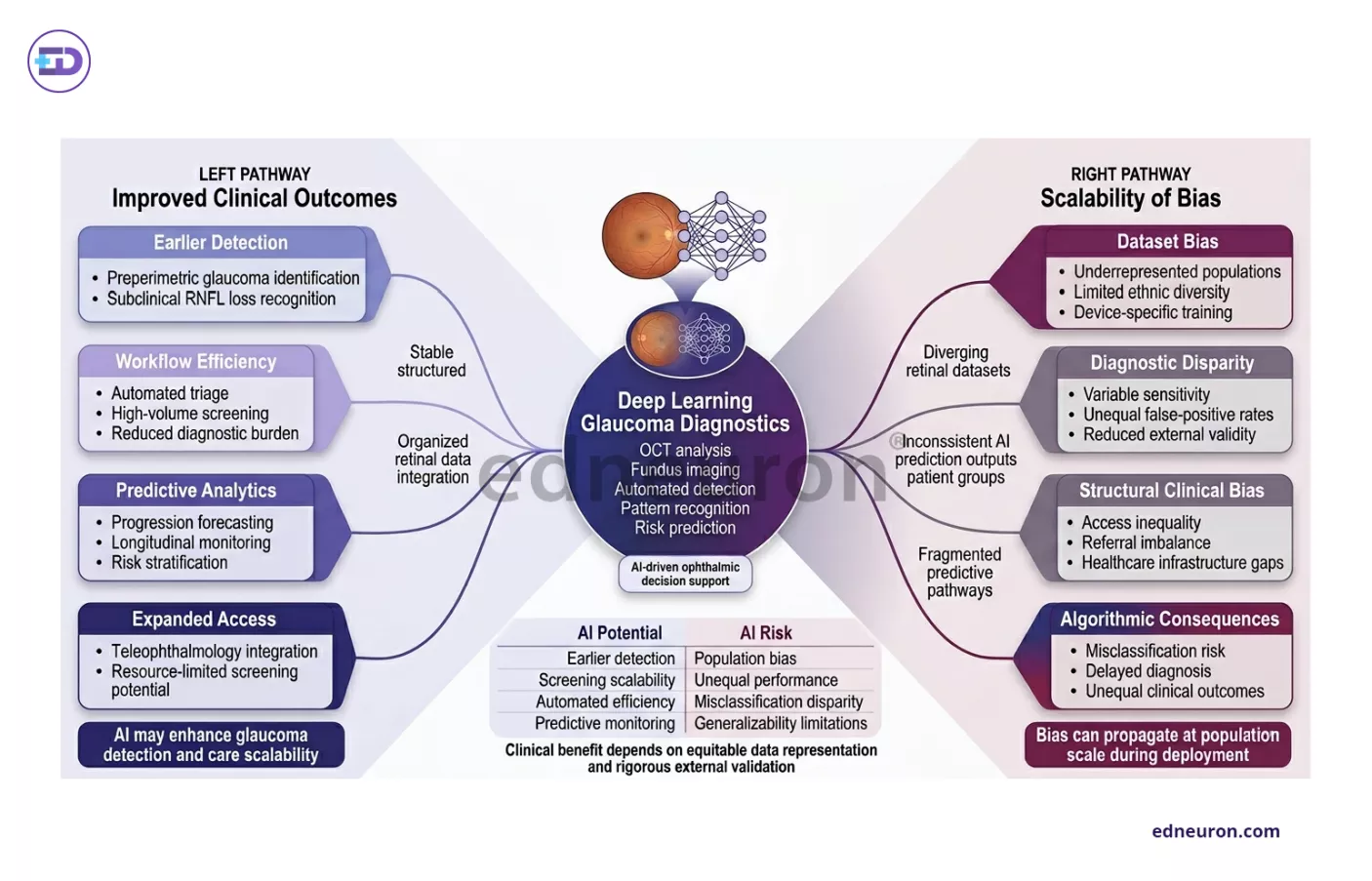
Fig 3: Deep learning may improve glaucoma outcomes at scale, but biased datasets can also propagate diagnostic inequities across diverse patient populations..
Clinical Outcomes and the Scalability of Bias
When DL models are used in real-world practice, they reveal new challenges related to patient differences. Evidence shows that popular models can unintentionally amplify existing human biases, leading to disparities in care. Large studies using the Ocular Hypertension Treatment Study (OHTS) dataset have found a “fairness gap,” where traditional DL models often underdiagnose younger female patients and overdiagnose older Black patients.
This shows that an algorithm’s strength depends on the diversity of its training data. A model trained on ideal, similar datasets often fails when used in real clinical settings with different imaging equipment or patient backgrounds. Also, while AS-OCT-based models perform very well for angle-closure detection in Asian populations, they are less useful for broader screening due to a lack of standardization across devices.
Conclusions
Deep learning in glaucoma is a major step forward in eye care, but it is not yet complete. Moving from manual checks to automated, multi-level analysis can help detect disease earlier, but clinical success depends on solving the following issues:
- Interpretability over Raw Accuracy: A diagnosis only matters in practice if it can be explained using anatomical knowledge through XAI.
- Mitigation of Algorithmic Bias: Future models need to focus on fairness across groups defined by combinations of race, sex, and age to avoid exacerbating healthcare disparities.
- Integration over Replacement: AI should function as a “clinician-in-the-loop” decision-support system, facilitating triage while specialists can focus on clinical management.
Ultimately, as we push past the measurement floor of traditional OCT, the goal is not merely a faster diagnosis, but a more equitable and transparent one.
References
- Ran AR, Tham CC, Chan PP, Cheng CY, Tham YC, Rim TH, et al. Deep learning in glaucoma with optical coherence tomography: a review. Eye (Lond). 2021 Jan;35(1):188-201. doi:10.1038/s41433-020-01191-5. Epub 2020 Oct 7. PMID: 33028972. PMCID: PMC7852526.
- Triolo G, Rabiolo A. Optical coherence tomography and optical coherence tomography angiography in glaucoma: diagnosis, progression, and correlation with functional tests. Ther Adv Ophthalmol. 2020;12:2515841419899822. doi:10.1177/2515841419899822. PMID: 32025510. PMCID: PMC6999543.
- Thompson AC, Jammal AA, Medeiros FA. Deep learning and optical coherence tomography in glaucoma: Bridging the diagnostic gap on structural imaging. Front Ophthalmol. 2022;2:937205. doi:10.3389/fopht.2022.937205.
- DINO-EYE Investigators. DINO-EYE: self-supervised learning for identification of different optic disc phenotypes in primary open angle glaucoma. Sci Rep. 2025;15:33140. doi:10.1038/s41598-025-33140-1.
- Yadav V, Dey B, Baruah U, Das S, et al. Machine learning-assisted image analysis techniques for glaucoma detection. EURASIP J Image Video Process. 2025;2025:68. doi:10.1186/s13640-025-00668-1.
- Abd El-Gawad AM, Hassan S, Elsharkawy M, et al. Explainable AI for glaucoma detection and classification: a comprehensive review. Artif Intell Rev. 2026;59:11551. doi:10.1007/s10462-026-11551-4.
- Thiery AH, Braeu F, Tun TA, Aung T, Girard MJA. Medical application of geometric deep learning for the diagnosis of glaucoma. arXiv [Preprint]. 2022 Apr 14:arXiv:2204.07004. doi:10.48550/arXiv.2204.07004.
- Lin M, Xiao Y, Hou B, et al. Evaluate underdiagnosis and overdiagnosis bias of deep learning model on primary open-angle glaucoma diagnosis in under-served patient populations. arXiv [Preprint]. 2023 Jan 26:arXiv:2301.11315. doi:10.48550/arXiv.2301.11315.
- Fu H, Xu Y, Lin S, Wong DWK, Baskaran M, et al. Angle-closure detection in anterior segment OCT based on multi-level deep network. arXiv [Preprint]. 2019 Feb 10:arXiv:1902.03585. doi:10.48550/arXiv.1902.03585.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



