

Introduction
In the management of invasive fungal infections, voriconazole remains a cornerstone therapy, yet its clinical application is notoriously bedeviled by a narrow therapeutic index and non-linear pharmacokinetics. Clinicians often find themselves chasing target trough concentrations (Co) in a “trial and error” loop, governed by dosing nomograms that frequently fail to account for the hidden variables of a patient’s biological landscape. What makes certain cases particularly challenging is not just the presence of a genetic variant or a single drug interaction, but the dynamic “masking” effect where one intervention inadvertently compensates for a genetic predisposition, only to reveal a clinical crisis when the medication regimen is altered. This case of a 35-year-old patient highlights the necessity of moving beyond standard dosing toward a sophisticated integration of pharmacogenetics and real-time therapeutic drug monitoring (TDM).
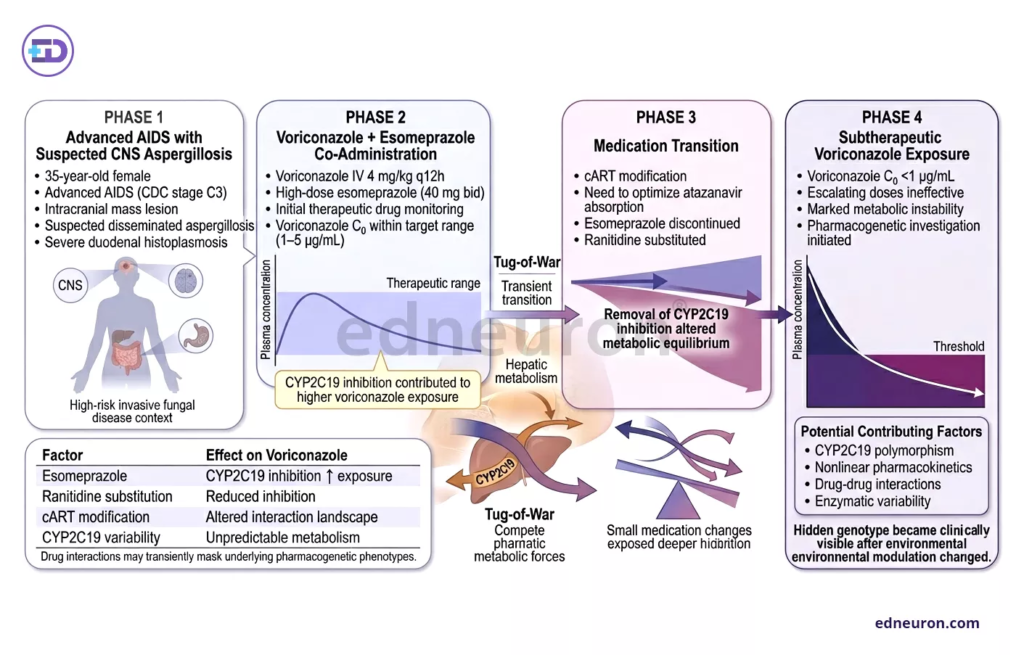
Fig 1 : Alteration of concomitant therapy unmasked profound pharmacogenetically mediated instability in voriconazole exposure despite therapeutic drug monitoring and dose escalation.
Case Presentation
A 35-year-old Cameroonian female with advanced AIDS (CDC stage C3) presented with a large intracranial mass of unknown origin. Suspecting disseminated aspergillosis, we initiated intravenous voriconazole at 4 mg/kg every 12 hours. Coincidentally, the patient was started on high-dose esomeprazole (40 mg bid) for severe epigastralgia related to duodenal histoplasmosis.
Initial TDM revealed voriconazole Co within the target range (1.0–5.0 μg/mL), which was reassuring. However, a transition in her antiretroviral therapy (cART) required swapping esomeprazole for ranitidine to facilitate atazanavir absorption. Within days of this switch, despite escalating the voriconazole dose, Co plummeted to subtherapeutic levels (<1.0 μg/mL). This metabolic instability prompted a deep dive into her pharmacogenetic profile and enzymatic “tug-of-war.”
Clinical Analysis
The central dilemma in this case was the dramatic loss of voriconazole exposure following a seemingly minor change in gastrointestinal prophylaxis. Voriconazole is primarily metabolized by CYP2C19 and, to a lesser extent, CYP3A4. The interpretation of this case hinges on the realization that the patient’s initial “therapeutic” levels were a pharmacological artifact.
Genotyping revealed she was heterozygous for the CYP2C19*17 allele, a variant associated with increased enzymatic activity, which is found in approximately 16% of African-Americans. Under normal circumstances, this “ultra-rapid” metabolizer status would result in persistently subtherapeutic levels. However, esomeprazole is a potent CYP2C19 inhibitor. By prescribing it for her epigastralgia, we had unintentionally “phenoconverted” her from an ultra-rapid metabolizer to a poor/intermediate metabolizer, effectively masking her genetic predisposition.
The uncertainty arose when ranitidine, which has no influence on CYP activity, was introduced. This “unmasked” her CYP2C19*17 hyperactivity. Even with the concurrent introduction of atazanavir, a CYP3A4 inhibitor, the uninhibited CYP2C19 pathway was so efficient that voriconazole clearance remained excessively high.
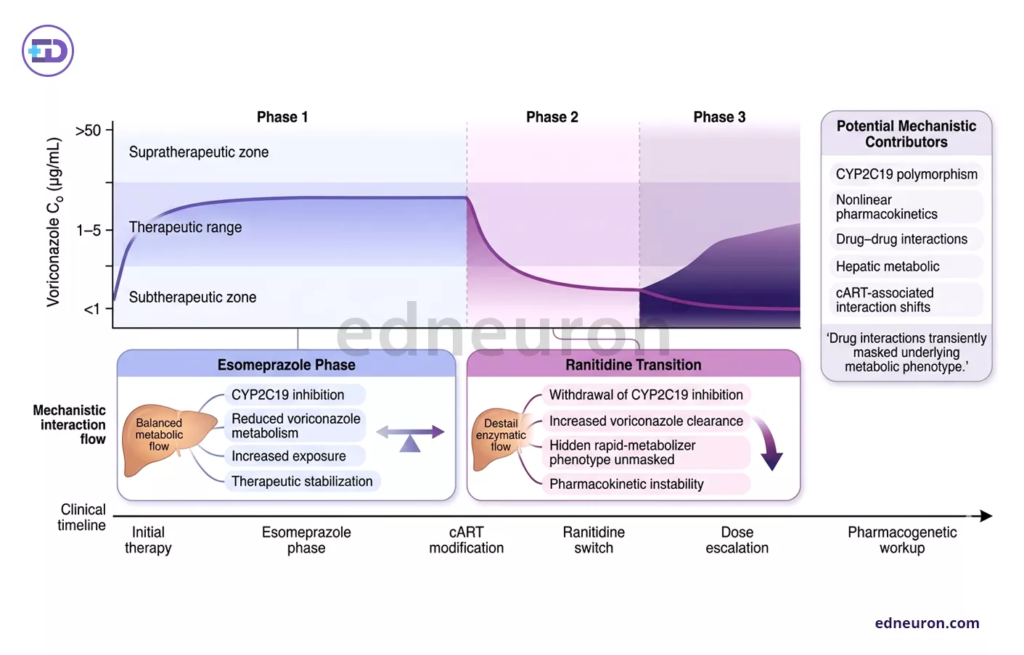
Fig 2 : Transition from esomeprazole to ranitidine unmasked profound CYP2C19-mediated instability in voriconazole exposure despite therapeutic drug monitoring and dose escalatio.
This phenomenon of concurrent influences is mirrored in other complex cases. For instance, in a report on apixaban, excessive exposure was not due to one factor but the convergence of moderate renal impairment and multiple functional polymorphisms in ABCB1 and CYP3A5. Similarly, our patient’s status was a net result of:
- Genetic Drive: CYP2C19*17 promoting rapid clearance.
- Pharmacological Brake: Esomeprazole inhibits that clearance.
- Secondary Modulation: Antiretrovirals (Atazanavir/Ritonavir) shifting the burden between the 2C19 and 3A4 pathways
Only by reintroducing esomeprazole did we achieve a “double blockade” of her metabolic pathways, finally stabilizing her voriconazole levels.
Clinical Implications
This case teaches us that TDM results must never be interpreted in a vacuum. A “therapeutic” level may be precarious, held in place by a specific drug-drug interaction (DDI) that, if removed, leads to immediate treatment failure.
In real-world practice, this suggests:
- Anticipatory Genotyping: In patients of ethnicities where CYP2C19*17 is prevalent (e.g., Caucasians ~21%, African-Americans ~16%), preemptive genotyping can alert clinicians to the need for higher doses or specific “boosting” strategies.
- The “Inhibitor-as-Stabilizer” Strategy: While we usually view DDIs as risks, this case illustrates they can be used strategically (similar to ritonavir boosting in HIV) to overcome high-clearance genotypes.
- TDM Frequency: Any change in PPIs or cART in a patient on voriconazole should trigger immediate TDM, as the “phenotype” can shift within 48–72 hours.
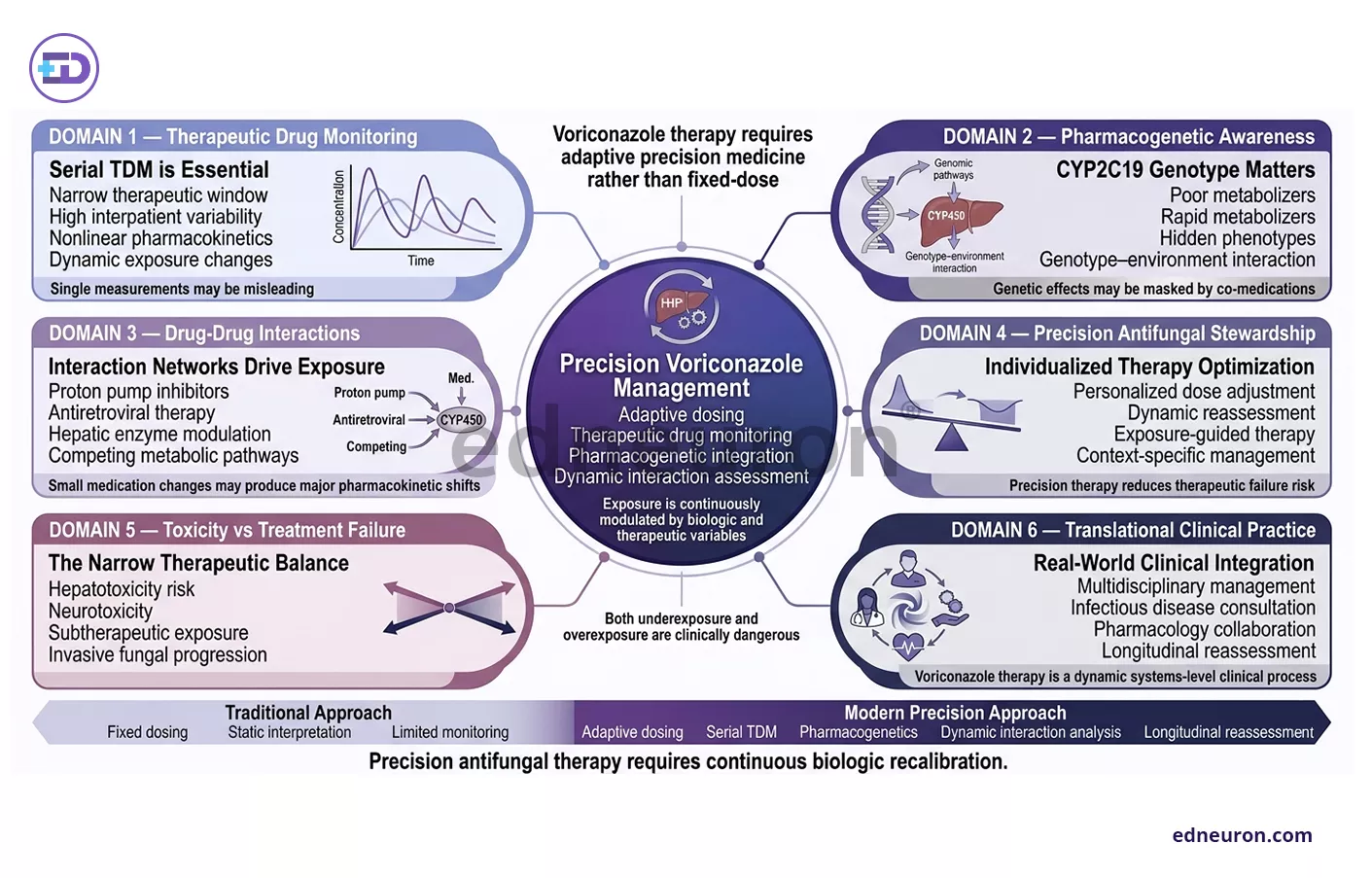
Fig 3: Effective voriconazole therapy requires continuous integration of pharmacogenetics, therapeutic drug monitoring, and dynamic interaction assessment to maintain safe and effective antifungal exposure.
Conclusions
The management of voriconazole in the critically ill requires an evolution from “standard of care” to “precision monitoring.” The patient in this vignette did not fail therapy because of a lack of drug; she failed because her underlying genetic “engine” was unmasked by a routine change in supportive care.
- Integrated Data is Key: Genetic data provides the blueprint, but DDIs provide the real-time operational status.
- Beyond Troughs: In pediatric or unstable cases, moving toward Area Under the Curve (AUC) measurements may provide a more stable marker of exposure than troughs alone.
- Clinical Vigilance: Always ask if a therapeutic level is being maintained by a “masking” agent that might soon be discontinued.
References
- Bouatou Y, Samer CF, Ing Lorenzini KR, Daali Y, Daou S, Fathi M, et al. Therapeutic drug monitoring of voriconazole: a case report of multiple drug interactions in a patient with an increased CYP2C19 activity. AIDS Res Ther. 2014;11:25. doi:10.1186/1742-6405-11-25. PMCID: PMC4135078. PMID:
- Chen J, Huang X, Lin Z, Li C, Ding H, Du J, et al. Case report: monitoring vancomycin concentrations and pharmacokinetic parameters in continuous veno-venous hemofiltration patients to guide individualized dosage regimens: a case analysis. Front Pharmacol. 2021;12:763575. doi:10.3389/fphar.2021.763575. PMID: 34955835. PMCID: PMC8695924.
- Duval X, Lemaitre F, Pertuisel S, Probert J, Gandemer V, Verdier MC, et al. The need for area under the curve measurements in the field of ganciclovir therapeutic drug monitoring in children: a case report. BMC Infect Dis. 2021;21(1):1143. doi:10.1186/s12879-021-06828-8. PMID: 34758818. PMCID: PMC8572521.
- Huppertz A, Grond-Ginsbach C, Dumschat C, Foerster KI, Burhenne J, Weiss J, et al. Unexpected excessive apixaban exposure: case report of a patient with polymorphisms of multiple apixaban elimination pathways. BMC Pharmacol Toxicol. 2019;20(1):53. doi:10.1186/s40360-019-0331-9. PMID: 31464657. PMCID: PMC6716843.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India


