

Abstract
Recent clinical trials have introduced shortened antituberculosis regimens for both drug-susceptible (DS-TB) and drug-resistant (DR-TB) disease. We have now 4-month rifapentine–moxifloxacin regimen demonstrating noninferiority to standard 6-month HRZE therapy in DS-TB, while bedaquiline–pretomanid–linezolid (BPaL) and BPaL-moxifloxacin (BPaLM)-based regimens achieve high treatment success rates in MDR/XDR-TB over just 6 months. These developments, even though they reflect a promising future, still face constraints on wider applicability when translating the trial results into practice. This article critically evaluates whether the newer shortened oral regimens represent a generalizable therapeutic advancement that promises the same favorable outcomes in endemic, high-burden areas or are the result of selective optimization contingent on patient eligibility, drug susceptibility, patient profiling, and infrastructure.
Introduction
Tuberculosis (TB) has long been distinguished among infectious diseases by its extremely distressing duration of longer treatment courses. The standard 6-month four-drug regimen-isoniazid, rifampicin, pyrazinamide, and ethambutol-established over decades of research, has remained the cornerstone of drug-susceptible TB management. Historically, for XDR/MDR TB, the imperative regimen suggesting 18-24 months duration therapy has long struggled with poor patient adherence and apprehension of second-line toxic injectables. The last 10 years have witnessed intensifying efforts to compress treatment duration without sacrificing efficacy.
Evidence
Dorman SE et al. reported that in DS-TB (drug susceptible TB), a 4-month regimen containing high-dose (1200mg) rifapentine and moxifloxacin was noninferior to standard 6-month HRZE therapy in a landmark phase III randomized controlled trial, with an adjusted absolute difference of 1.0 percentage point (95% confidence interval [CI], −2.6 to 4.5). This finding, supported by multicenter data, led to revisions in both the World Health Organization (WHO) and the ATS/CDC/ERS/IDSA guidelines, which recommend the 4-month regimen for eligible patients. The Nix-TB study and ZeNix phase II/III trial also provide sufficient evidence of advances in MDR/XDR TB. The BPaL regimen demonstrated high cure rates and more rapid sputum conversion in XDR/MDR TB over a 6-month period. A lower dose of linezolid (600 mg) was associated with an improved safety profile. Subsequent evidence-based research has extended these findings to individualized, shorter oral regimens, demonstrating noninferiority across diverse patient populations.
Mechanistic And Pharmacologic Rationale
The pharmacologic rationale for treatment shortening is based on the properties of drug synergy and sterilizing efficacy. Bedaquiline inhibits mycobacterial ATP synthase, disrupting the energy production in live and dormant bacterial populations. Pretomanid is a nitroimidazole active against both actively replicating bacteria by inhibiting mycolic acid synthesis and in dormant non-replicating populations by nitric oxide release. Linezolid works by inhibiting ribosomal subunits, making it particularly effective against highly resistant organisms. In drug-susceptible tuberculosis (DS-TB), we achieved better patient compliance by replacing rifampicin with rifapentine. Rifapentine’s extended half-life compared to rifampicin allows for once daily dosing. However, rifamycins are associated with hepatotoxicity and hyperbilirubinemia, necessitating strict monitoring. Moxifloxacin, which replaces ethambutol, offers independent bactericidal activity. This combination allows for a shorter treatment duration while maintaining non-inferiority to existing regimens.
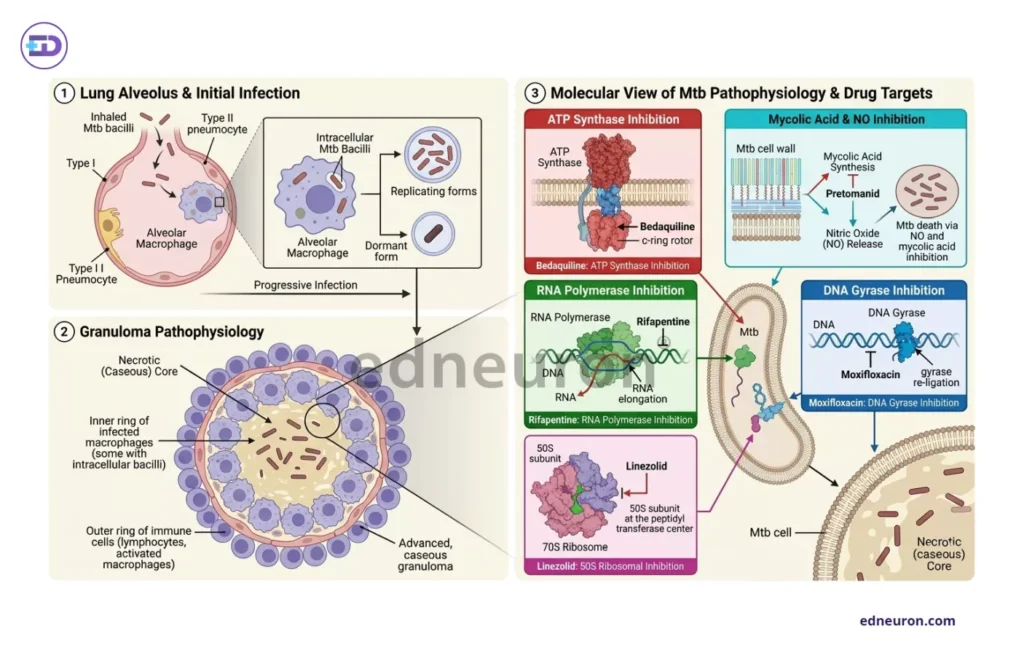
Fig 1: Illustration of the pathophysiology of Mycobacterium tuberculosis and the molecular target sites of various antitubercular drugs.
Critical Appraisal
Several factors merit consideration amidst the enthusiasm surrounding the shorter oral regimen.
- Linezolid-related toxicity-myelosuppression, peripheral neuropathy, and optic neuritis-is dose- and duration-dependent. It emerged as a primary determinant of both efficacy and tolerability in the ZeNix trial, where lower linezolid doses (600 mg vs. 1200 mg) over 26 weeks reduced adverse events without significant loss of efficacy. The one thing this safety-efficacy trade-off requires is the capacity for prospective monitoring, which may be unavailable in high-burden, resource-limited settings. Although the shorter regime showed promising results, the added costs for quicker outcomes do not entirely alleviate the problem in high-burden, low-income countries.
- Emerging resistance to bedaquiline and pretomanid-mediated by mutations in atpE, pepQ, fgd1, and ddn, raises important questions regarding the long-term durability of current regimens in settings with elevated transmission pressure. What these shorter regimens do is accelerate the drug exposure, which risks selection of mutant varieties under sub-optimal adherence.
- WHO-Europe’s multinational observational cohort (across 13 nations) reported approximately 83% treatment success with 9-month MDR-TB regimens. While this is indeed encouraging, the reality falls below clinical trial benchmarks, highlighting stagnation in implementation pipelines. The compounding heterogeneity in disease burden, HIV co-infection, and comorbidities does not help the case of the generalizability of trial-derived noninferiority margins.
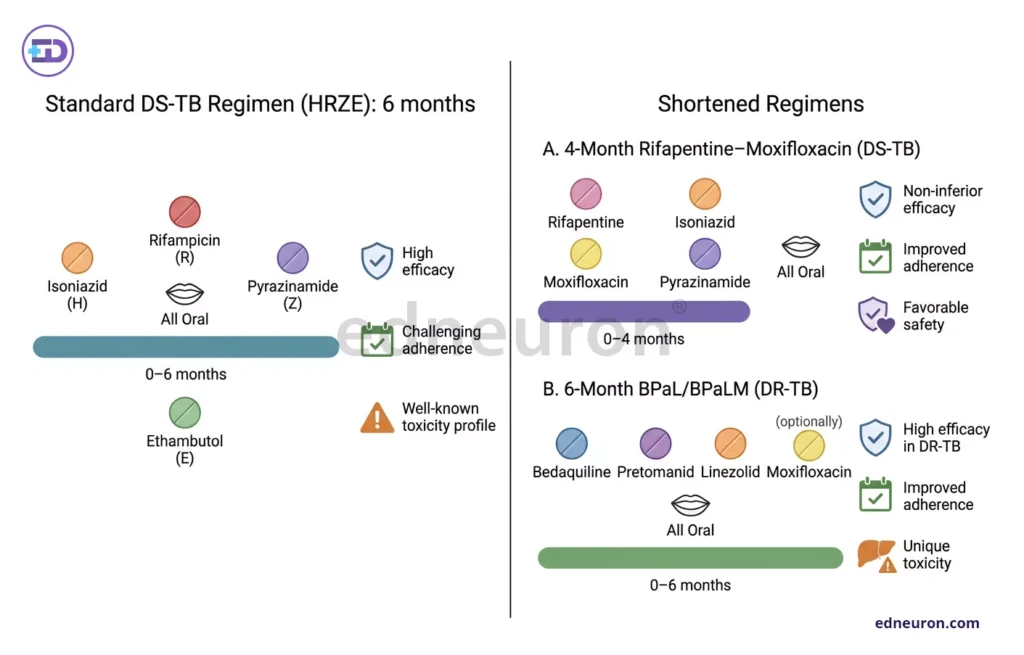
Fig 2: Implementation in newer drug therapy heralds not only favorable outcomes and improved adherence but also unique toxicity drug profiles in a varied population.
Future Directions
The endTB-Q trial’s results, which show that personalized 6 to 9 month regimens can achieve strong outcomes in difficult-to-treat TB subsets, reflect that the future of TB treatment lies not in generalizing a predefined regimen but in individualizing drug therapy to suit patients’ disease profiles, susceptibilities, and tolerability. Integration of whole-genome sequencing for rapid resistance profiling and emerging computational approaches to regimen optimization, including AI-assisted drug combination prediction, may enable more precise matching of regimen intensity and duration to individual disease burden and pharmacogenomic profile. It is also important to note that in the Tuberculosis Trials Consortium Study 31 demonstrated that the surrogate biomarker to assess antimicrobial activity (sputum conversion to negative culture) differed very little among the rifapentine-moxifloxacin vs rifapentine only. Such evidence suggests the need for better-validated biomarkers to determine early treatment response, which may prospectively guide decisions on treatment duration.
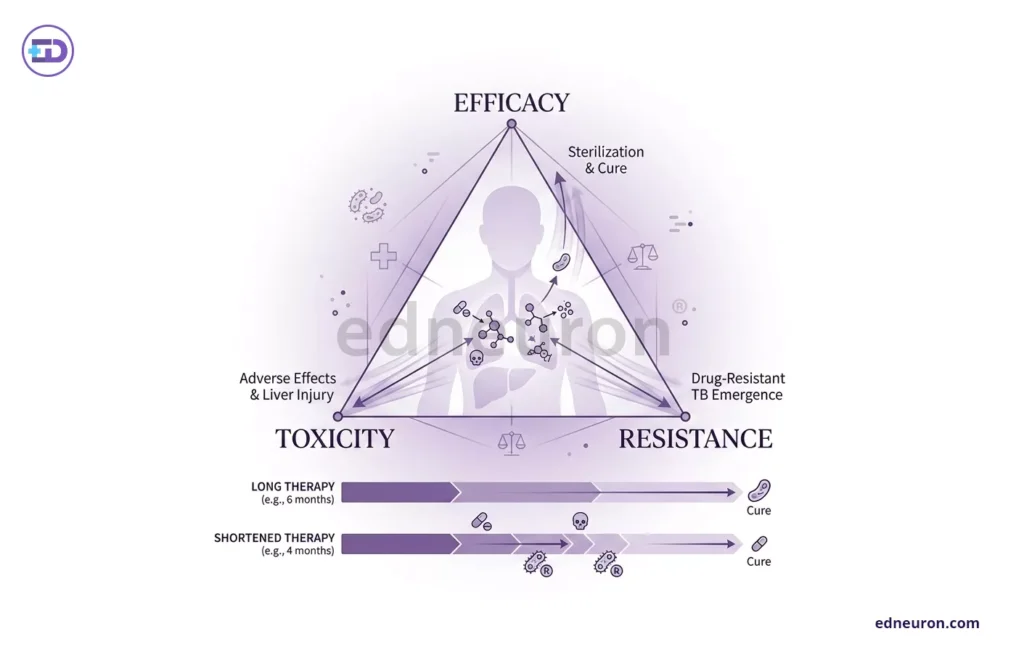
Fig 3: Generalizability of any therapy should not just be a byproduct of comparative cure rates in a shorter time but an ultimate solution that weighs all parameters and acknowledges the crucial tension in terms of toxicity, efficacy, and emerging resistance.
Conclusion
Although the evidence supporting shortened antituberculosis regimens is ample and irrefutable, it does not constitute a common solution without conditions. We saw that for DS-TB, the 4-month rifapentine–moxifloxacin regimen represents a well-validated modification and in DR-TB, BPaL and BPaLM regimens have replaced poorly tolerated injectable courses with shorter, all-oral alternatives of demonstrated efficacy. These are meaningful achievements, yet the qualifying conditions-patient eligibility, susceptibility, toxicity-monitoring capacity, resistance surveillance, and programmatic infrastructure-are not merely external constraints but rather the inherent determinants that dictate the success of such research trials. Shortened TB therapy represents, at present, selective optimization: transformative for those who qualify, and a challenge still unmet for the many who do not.
References
- Dorman SE, Nahid P, Kurbatova EV et al.; AIDS Clinical Trials Group; Tuberculosis Trials Consortium. Four-Month Rifapentine Regimens with or without Moxifloxacin for Tuberculosis. N Engl J Med. 2021 May 6;384(18):1705-1718. PMID: 33951360.
- World Health Organization. WHO consolidated guidelines on tuberculosis: module 4: treatment and care. 2025.
- Infectious Diseases Society of America. ATS/CDC/ERS/IDSA treatment of drug-susceptible and drug-resistant TB: 2025 update.
- Conradie F, Bagdasaryan TR, Borisov S et al.; ZeNix Trial Team. Bedaquiline-Pretomanid-Linezolid Regimens for Drug-Resistant Tuberculosis. N Engl J Med. 2022 Sep 1;387(9):810-823. PMID: 36053506.
- Oelofse S, Esmail A, Diacon AH et al. Pretomanid with bedaquiline and linezolid for drug-resistant TB: a comparison of prospective cohorts. Int J Tuberc Lung Dis. 2021 Jun 1;25(6):453-460. PMID: 34049607
- endTB trial. Phase III randomized controlled trial results.
- endTB-Q trial. Landmark results published in Lancet Respiratory Medicine.
- WHO/Europe. Shorter TB treatment regimen shown to be safe and effective in operational research. June 2024.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi


