Introduction
Neonatal hypoxic-ischemic encephalopathy (HIE) is a highly debilitating condition often as a result of perinatal asphyxia affecting about 3/1000 live births, especially in the middle- and low-income countries than in the developed world. The two main culprits are reduced cerebral blood flow and anoxic injury to the brain, especially in pregnancies with intrapartum complications. On the molecular level, we can categorize it as a cascade of 2 phases: Primary energy failure with a fall in ATP due to decreased oxidative phosphorylation, and reperfusion injury (latent phase), characterized by glutamate excitotoxicity, free radical injury, and caspase activation. Studies show that the latency period, often marked at 6 hours from birth, is the most pivotal factor predicting the course of injury.
Mechanism of Therapeutic Hypothermia
So the question is, how does cooling the brain actually reduce brain injury? One might think it miraculous, but the mechanism becomes intuitive when one imagines how temperature affects our basal metabolism. Neuroprotection is achieved by reducing cerebral metabolic rate, free radical generation, and oxygen demand, and by lowering the activity of biosustaining enzymes at a target temperature of 33-34°C, thereby preserving neuronal viability during the latent phase. Cooling reduces mortality without increasing major disability in survivors.
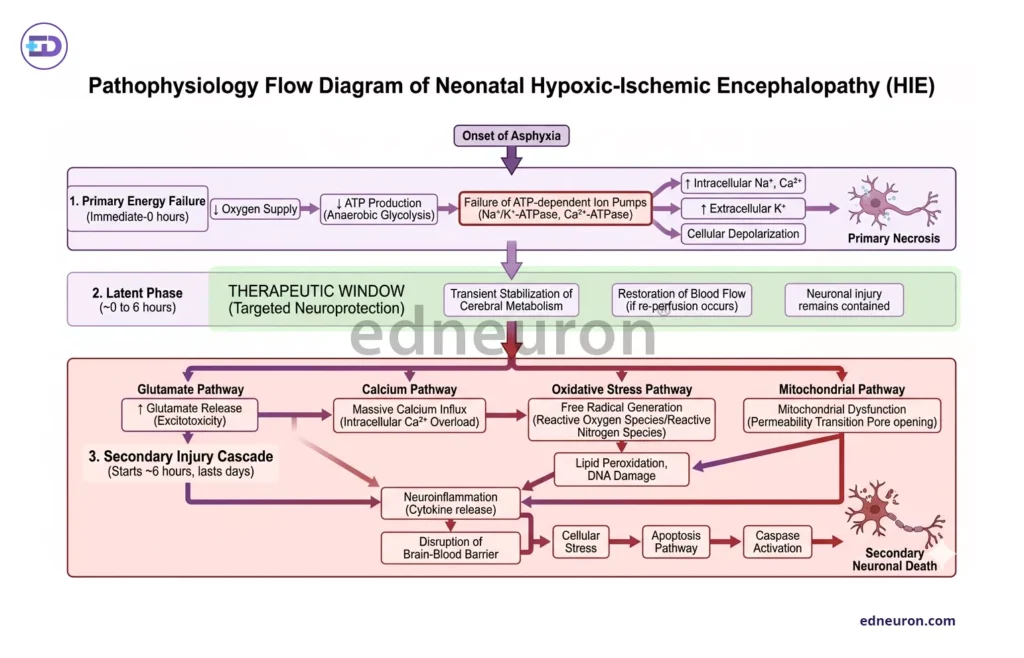
Fig 1: Illustration of the pathophysiology of HIE and the importance of acting before the latent phase progresses into secondary neuronal damage.
Indications
This is indicated in neonates meeting the following criteria:.
- Gestational age ≥36 weeks (preterms contraindicated- high risk for hypoglycemia and other complications)
- Age ≤6 hours
- Birthweight > 1800 grams
- Evidence of moderate-to-severe encephalopathy.
- Clinical: Apgar score ≤5 at 10 minutes, continued need for resuscitation.
- Cord pH <7.0 / base deficit ≥16 mmol/L.
- Biochemical: Arterial pH <7.0 or lactate >12 mmol/L.
- Neurological staging: Sarnat grade II (moderate) or III (severe) encephalopathy.
How do we do it?
There are two main approaches: either we selectively cool the head using a cooling cap or place a cooling blanket, which indirectly cools the brain. Will it not increase the risk of hypothermia? For that, the core temperature must be continuously measured using probes in the esophagus or rectum. Modern cooling systems are automated to adjust the temperature of circulating water in the blanket to maintain a stable target temperature. With proper monitoring, this can be an exceptionally important implication of preventative neonatal medicine.
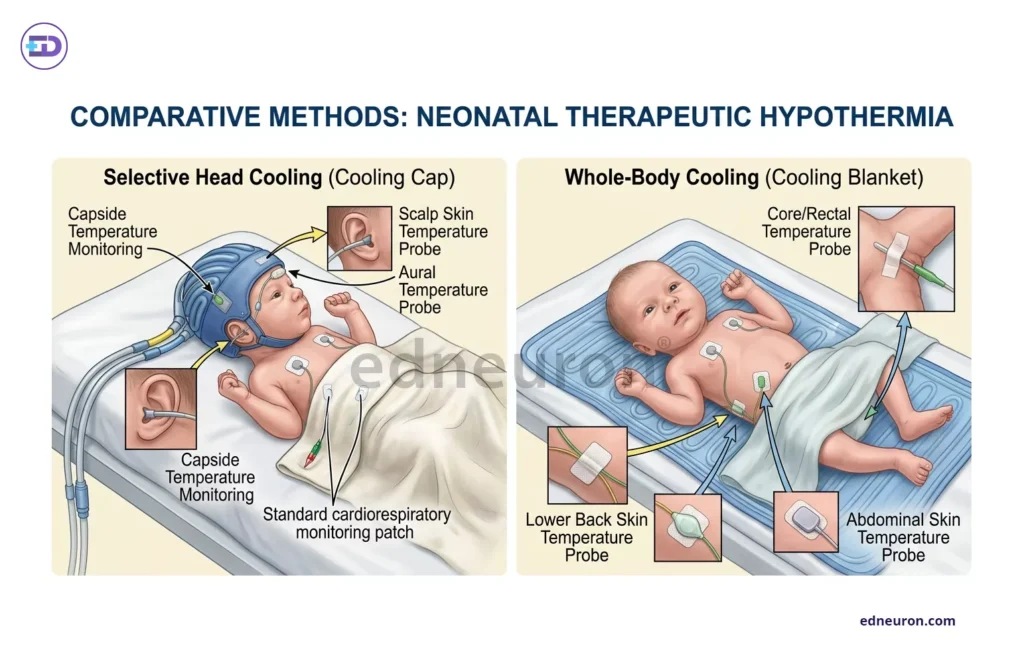
Fig 2: The first panel shows selective head cooling, whereas second panel describes cooling blanket mechanism which is now more widely used than the former.
Clinical Outcomes
Meta-analysis by Tagin et al. (2012) pooled data from 7 randomized controlled trials (n=1,214) and demonstrated that TH significantly reduced the outcome of mortality and neuronal debilitation in moderate-to-severe HIE (RR 0.76; 95% CI 0.69–0.84). A 2022 systematic review supported these findings, i.e., improved survival and favorable neurodevelopmental trajectories — including reduced cerebral palsy and cognitive impairment — at 18–24-month follow-up. The number needed to treat is 7 underscores TH as one of the most impactful interventions in neonatal medicine. However, it is worth mentioning that newborns who are asphyxiated beyond compensation are unlikely to benefit from hypothermic therapy. So two things become indispensable-
- Prompt intervention before the secondary phase
- Identifying newborns who are beyond the window of opportunity is therefore essential; so is vigilance for non-responders.
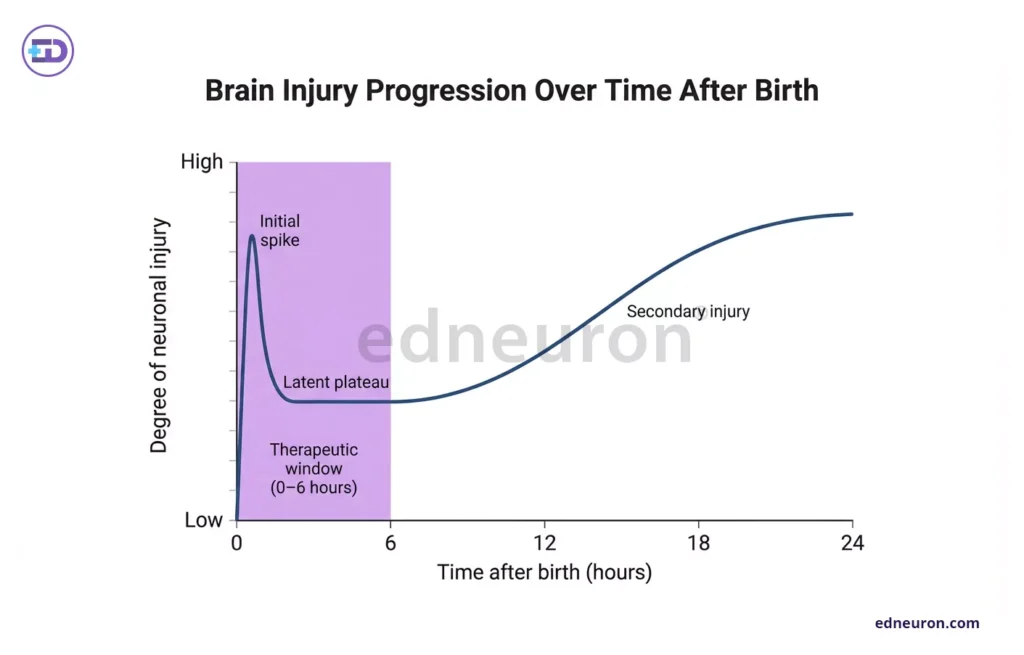
Fig 3: The therapeutic window is indispensable in reversing brain injury and reducing the chances of cerebral palsy.
References
- Jennifer J. Kurinczuk, Melanie White-Koning, Nadia Badawi, Epidemiology of neonatal encephalopathy and hypoxic–ischaemic encephalopathy, Early Human Development, Volume 86, Issue 6, 2010, Pages 329-338, ISSN 0378-3782, PMID: 29265370.
- Jacobs S, Hunt R, Tarnow-Mordi W, Inder T, Davis P. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev. 2007 Oct PMID: 17943788.
- Arnautovic T, Sinha S, Laptook AR. Neonatal Hypoxic-Ischemic Encephalopathy and Hypothermia Treatment. Obstet Gynecol. 2024 Jan PMID: 37797337.
- Mathew JL, Kaur N, Dsouza JM. Therapeutic hypothermia in neonatal hypoxic encephalopathy: A systematic review and meta-analysis. J Glob Health. 2022 Apr PMID: 35444799.
- Laptook AR, Shalak L, Corbett RJ. Differences in brain temperature and cerebral blood flow during selective head versus whole-body cooling. Pediatrics. 2001;108:1103–10 [PubMed:11694688]
- Tagin MA, Woolcott CG, Vincer MJ, Whyte RK, Stinson DA. Hypothermia for Neonatal Hypoxic Ischemic Encephalopathy: An Updated Systematic Review and Meta-analysis. Arch Pediatr Adolesc Med. 2012;166(6):558–566.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi