
Introduction
The presentation of sensorineural or conductive hearing loss along with episodic or sustained vertigo constitutes one of the most nuanced scenarios in clinical otolaryngology. The coexistence of these two symptoms effectively narrows the localization to the inner ear (labyrinth) or the vestibulocochlear nerve (CN VIII), since both the auditory and vestibular end organs are encased within the same otic capsule and share common fluid compartments. Peripheral causes dominate the differential over the central etiologies. Four conditions account as differentials and pose the greatest challenges:
- Ménière’s disease (endolymphatic hydrops),
- Superior Semicircular Canal Dehiscence (SSCD; third-window pathology)
- Labyrinthitis (viral or bacterial inflammation)
- Perilymph Fistula (PLF; abnormal perilymph leakage).
Their shared symptom complex, hearing loss with vertigo, demands a structured rather than intuitive diagnostic approach.
Pathophysiology: Mechanism-Based Distinctions/ Differentials
- Endolymphatic Hydrops (Ménière’s Disease)
Ménière’s disease characterizes excessive accumulation of endolymph within the membranous labyrinth- a state termed endolymphatic hydrops. Primary cause is mostly idiopathic, whereas secondary causes can be attributed to infection, trauma, allergy, autoimmune conditions, and, in some rare cases, genetic conditions. The most widely accepted hypothesis implicates impaired resorption of endolymph by the endolymphatic sac, resulting in distension of the saccule and cochlear duct (scala media). The resulting increase in endolymphatic pressure is thought to cause first bulging of Reissner’s membrane followed by periodic ruptures, allowing potassium-rich endolymph to mix with sodium-rich perilymph, depolarising vestibular and cochlear hair cells the putative reason for episodic attacks of vertigo and hearing loss. One key feature is hearing loss, which is gradually progressive due to repeated damage to hair cells that fluctuates. Peculiarly, the apex of the cochlea is affected first, causing marked low-frequency hearing loss. cycle of rupture and repair. The patient also complains of aural fullness and tinnitus. Gadolinium-enhanced 3T MRI (3D-FLAIR protocol) after intratympanic or intravenous Gd administration can now visualize endolymphatic hydrops in vivo, lending histological and mechanical plausibility to this theory. - Third-Window Effect (SSCD)/ Superior Semicircular Canal Dehiscence.
The inner ear snugly fits into a bony canal called the bony labyrinth, communicating with the middle ear through the oval window (stapes footplate) and the round window, and with the brain through the Inner acoustic meatus and cochlear aqueducts. Superior Semicircular Canal Dehiscence creates an aberrant third compliant interface between the inner ear and the middle cranial fossa (arcuate eminence). First described by Lloyd B. Minor and colleagues at Johns Hopkins in 1998, SSCD allows acoustic energy and pressure changes to bypass the normal cochlear partition pathway. Acoustic emissions entering via the oval window is “short-circuited” or lost through the dehiscent canal, simultaneously reducing cochlear drive/stimulation (mimicking conductive hearing loss) and pathologically exciting the superior semicircular canal hair cells (inducing vertigo and vertical nystagmus along with torsion). Hearing loss is pseudo-conductive: low-frequency air-bone gap with normal acoustic reflexes and supranormal BC thresholds. Autophony is one of the most pathognomonic clues for SSCD-Hearing one’s own voice, heartbeat, or eyeball movements, or footsteps. - Inflammatory Labyrinthitis
Labyrinthitis results from inflammatory infiltration of the membranous labyrinth. Common causes include- Viral labyrinthitis (most commonly by HSV-1, mumps, CMV, or upper respiratory viruses) either caused by direct viral injury or immune-mediated damage to cochlear and vestibular hair cells.
- Bacterial labyrinthitis (suppurative), a serious complication of otitis media or meningitis, may result in complete unilateral hearing loss and carries a risk of intracranial extension through the internal acoustic meatus.
- Serous labyrinthitis arises from inflammatory toxin infiltration without direct bacterial invasion, a critical distinction with therapeutic implications.
Unlike SSCD and Ménière’s disease, labyrinthitis destroys end-organ function rather than producing reversible biomechanical perturbations, thereby explaining the typically persistent, rather than episodic, vestibular deficit.
- Perilymph Fistula (PLF)
A PLF is an abnormal communication between the perilymph-filled inner ear spaces and the air-filled middle ear, most commonly through rupture of the oval or round window membranes. Either through- Trauma (bony erosions due to cholesteatoma due to unsafe CSOM)
- Iatrogenic cause (stapedotomy, modified radical mastoidectomy)
- Barotrauma leading to round window rupture.
Loss of perilymph integrity disrupts the normal closed-fluid mechanics of the cochlea; the addition of a third compliant window, whether or not frank leakage occurs, may alter the propagation of fluid waves through the labyrinth, producing sound- or pressure-induced cupular deflection and vertigo.
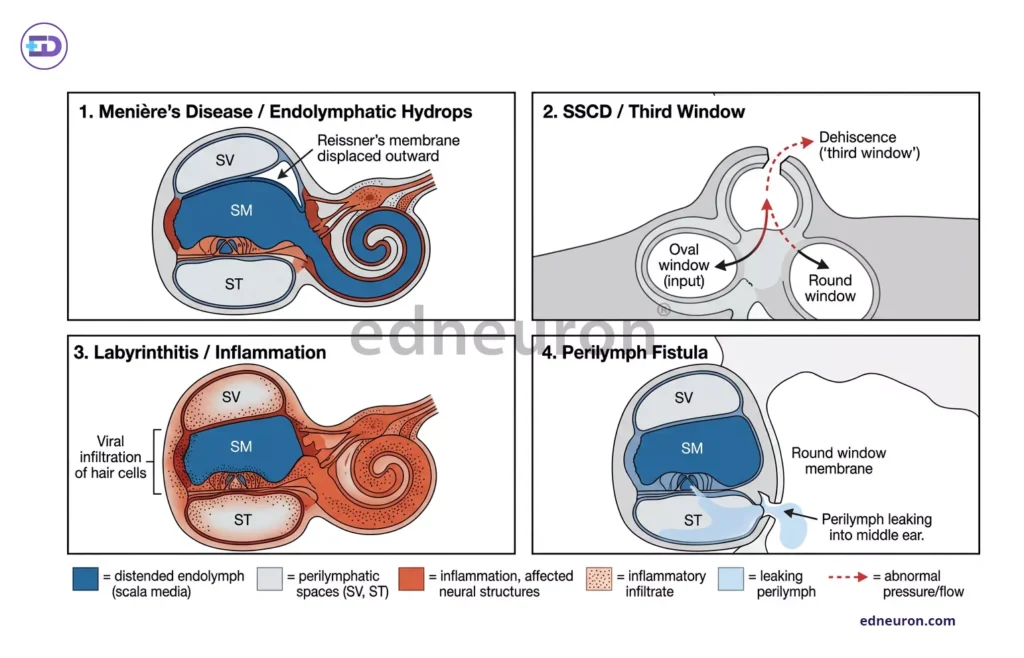
Fig 1: Comparative panel of pathophysiology of various differentials.
Diagnostic Framework
Step 1
Patients present with complaints of Deafness + Vertigo →
- Localize to the peripheral inner ear (labyrinth ± CN VIII).
- Central cause- if focal neurological signs, new-onset headache, or crossed deficits. Or nystagmus that has no latency/no fatiguability/ which persists on optic fixation using Frenzel goggles
STEP 2
Is vertigo acute, severe, and continuous? Along with the duration of vertigo.
- Onset- Spontaneous, no identifiable trigger with episodic vertigo attacks: 20 min – 12 hours per attack along with vagal symptoms like nausea, vomiting, diarrhea, abdominal cramps, and bradycardia-Ménière’s Disease
- Onset-Often insidious; may follow head trauma or rapid pressure change. Vertigo- Triggered by loud sounds (Tullio phenomenon) or Pressure changes.
- Onset- Acute (often following viral URTI or acute otitis media); bacterial form associated with meningitis. Vertigo- Severe, acute, continuous (not episodic)→ Labyrinthitis
- Onset-Post-barotrauma, head trauma, Valsalva, lifting, or idiopathic vertigo-Pressure-induced (straining, nose-blowing, coughing)–Perilymphatic Fistula.
Step 3
Assess Hearing loss and associated symptoms.
- SNHL (sensorineural hearing loss)- Ménière’s Disease/ Perilymphatic Fistula/Labyrinthitis
- CHL(conductive hearing loss)- SSCD
Investigations: Audiological and Radiological Findings
PURE TONE AUDIOMETRY (PTA)
- Low-frequency SNHL (250–1000 Hz)- Classic for Ménière’s
- Pseudo-conductive pattern is pathognomonic for SSCD
- Profound flat SNH- Suggests suppurative labyrinthitis
- Supranormal bone conduction BC- thresholds below 0 dB HL- classic SSCD.
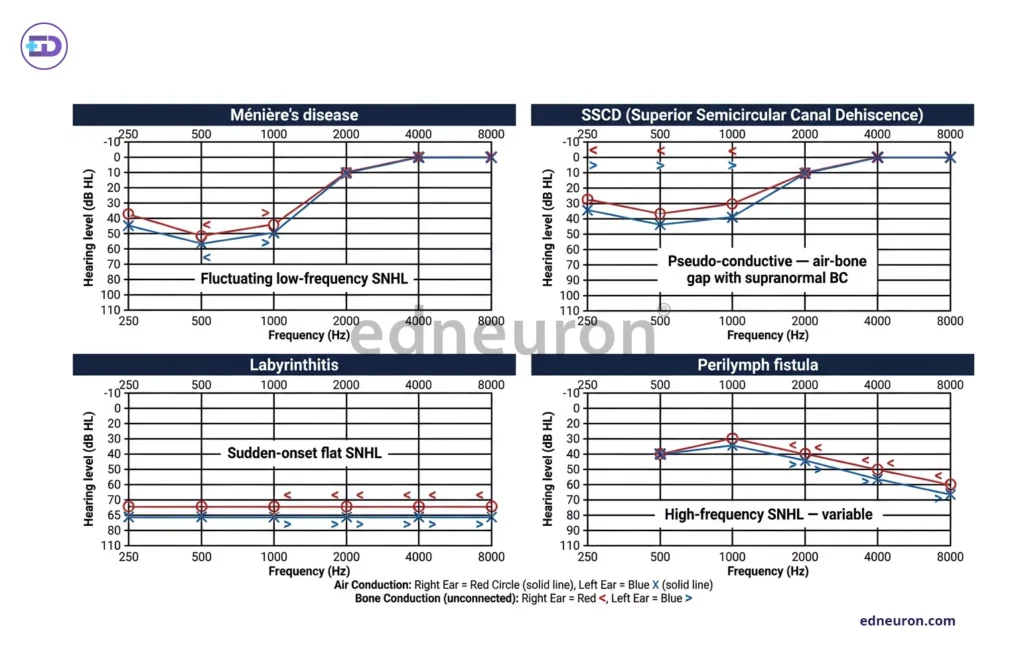
Fig 2: Comparative panel of Audiograms.
ELECTROCOCHLEOGRAPHY (ECochG)
- Elevated SP: AP ratio (>0.4) indicates endolymphatic hydrops in Ménière’s disease
- Reversible ECochG changes in SSCD may normalise after plugging surgery
- Used in surgical monitoring, Intraoperative ECochG during SSCD repair to preserve hearing
HIGH-RESOLUTION CT TEMPORAL BONE
- Pöschl’s view (in-plane SCC) confirms bony dehiscence over the superior canal in SSCD
- Stenvers view (orthogonal), complementary to Pöschl; must use 0.6 mm slice thickness
- Normal CT with SSCD symptoms “Near dehiscence” -thin but intact bone can still produce symptoms
- Labyrinthine air or window defects-Suggestive of PLF; requires clinical correlation
MRI (GADOLINIUM-ENHANCED, 3T)
- 3D-FLAIR post-IV/IT Gd (4–24h delay)- Visualizes endolymphatic hydrops in Ménière’s- perilymphatic space, non-visualized.
- Labyrinthine enhancement indicates viral/inflammatory labyrinthitis.
- PLF detection-MRI may show perilymphatic fistula; CT/MRI together yield higher sensitivity
CALORIC / VIDEO HEAD IMPULSE TESTING (vHIT)
- Caloric: canal paresis- reduced or absent response corresponds to labyrinthitis or end-stage Ménière’s
- vHIT-gain reduction: Selective for each SCC; identifies remaining vestibular function
- Tullio/fistula response: Pressure-induced nystagmus/vertigo seen in PLF and occasionally Ménière’s Sound or pressure-induced nystagmus in the plane of superior SCC → SSCD
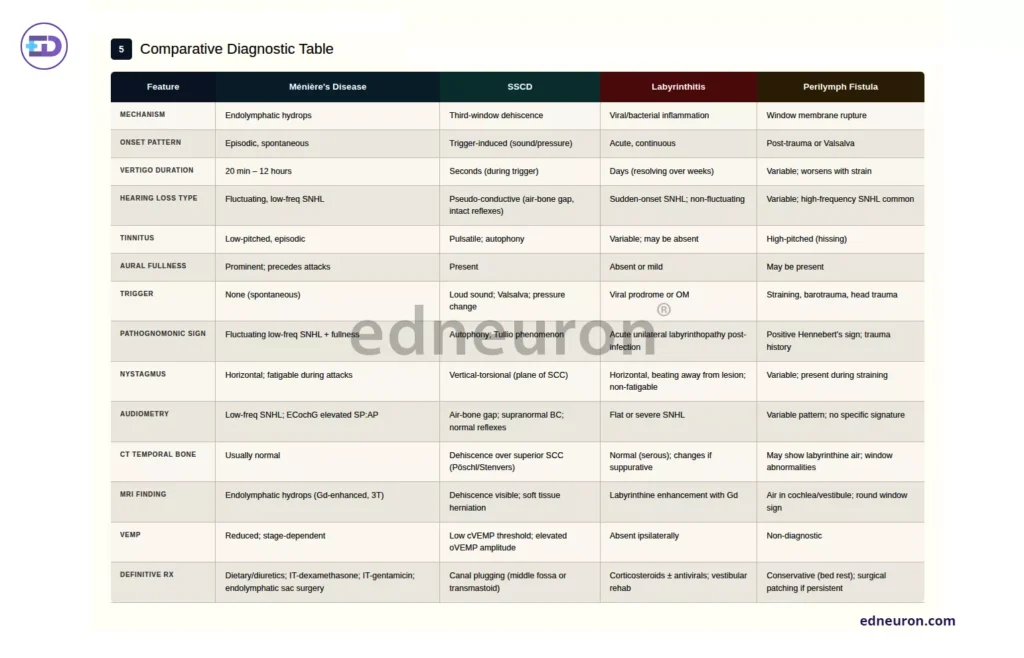
Fig 3: Comparative Diagnostic Table- summary of numerous signs and symptoms.
References
- Watkinson JC, Clarke RW, editors. Scott-Brown’s Otorhinolaryngology Head and Neck Surgery. 8th ed. Boca Raton: CRC Press; 2018. Chapter: Vestibular disorders and inner ear pathology.
- Flint PW, Haughey BH, Lund VJ, et al., editors. Cummings Otolaryngology — Head and Neck Surgery. 7th ed. Philadelphia: Elsevier; 2021. Chapter 163: Labyrinthitis and inner ear inflammatory disorders.
- Flint PW, et al. Cummings Otolaryngology — Head and Neck Surgery. 7th ed. Philadelphia: Elsevier; 2021. Chapter 165: Meniere’s disease and endolymphatic hydrops. [Chapter reference]
- Minor LB, Solomon D, Zinreich JS, Zee DS. Sound- and/or Pressure-Induced Vertigo Due to Bone Dehiscence of the Superior Semicircular Canal. Arch Otolaryngol Head Neck Surg. 1998;124(3):249–258.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi


