

Introduction
A 58-year-old man with poorly controlled diabetes presents to the emergency department with two days of fever, rigors, and malaise. His blood pressure reads 118/74 mmHg; his heart rate is 102 beats per minute. The triage nurse categorizes him as non-urgent. Thirty minutes later, his serum lactate returns at 5.2 mmol/L. He has no hypotension. He is, by conventional vital sign triage, ‘stable.’ Is he?
This vignette illustrates one of the most perplexing paradoxes of emergency medicine, in which the clinician equates optimal blood pressure with adequate perfusion. The concept of cryptic shock, defined as normotension with serum lactate≥ 4 mmol/L, has been found to have an in-hospital mortality similar to that of overt shock (21%) (Puskarich MA et al. 2011). This highlights the need to integrate such a phenotype into sepsis resuscitation protocols. If a clinician labels such a patient in cryptic shock as stable, it’s almost akin to losing the very precious critical window that can save a life.
Why Vital Signs Mislead
Blood pressure is a macrocirculatory variable- the product of cardiac output and systemic vascular resistance. Such a global hemodynamic summary tells us nothing about whether the individual organs and microvascular beds are receiving adequate oxygen. In early sepsis, compensatory mechanisms of the body, such as vasoconstriction, tachycardia, and neurohormonal activation, may maintain systemic pressure. This does not guarantee that microvascular flow will remain homogeneous and adequate. This macro–microcirculatory decoupling is directly measurable at the bedside and has been demonstrated reproducibly in experimental and clinical sepsis models. Mikkelsen ME et al. demonstrated in a retrospective cohort of 830 patients that intermediate lactate elevation (2-3.9) was associated with a graded increase in mortality, independent of organ failure score and shock status, among patients with cryptic shock, proving that the nonshock, normotensive subgroup carries significant prognostic risk.
Pathophysiology- Pressure Is Preserved, but Perfusion Is Not
The cellular pathophysiology of sepsis involves broadly three interrelated mechanisms that operate independently of macrohemodynamic parameters.
- Microcirculatory dysfunction
Microcirculatory vessels include arterioles, venules, capillaries, and microlymphatics, and contain a diverse array of cells, including endothelial cells, smooth muscle cells, RBCs, WBCs, and platelets. During sepsis, there is a breakdown of endothelial regulation, characterized especially by heterogeneity in iNOS (inducible NOS) expression. This shunts blood from regions deficient in iNOS, leading to greater hypoperfusion. Also, the hemoglobin has reduced capacity to release vasodilators, further compounding the effect during hypoxia. Reduced deformability, increased adhesin expression, and neutrophil trafficking all increase the aggregability of these cells, which, when compounded with platelet dysfunction and glycocalyx breakdown, lead to increased procoagulant and prothrombotic states. This is not corrected by normalizing blood pressure alone. - Endothelial injury drives systemic inflammation, coagulation activation, and vascular leak, adding to tissue hypoperfusion even when cardiac output remains preserved.
- Mitochondrial dysfunction, so-called cytopathic hypoxia. Here, elevation in lactate levels does not just signify anaerobic glycolysis but the very inability of cells to utilize oxygen. While being a clinically accessible marker, it also serves as a great prognosticating factor. A 2025 prospective study confirmed that lactate clearance is an independent predictor of mortality, ICU length of stay, and vasopressor requirements. Moreover, the recommendation mentions that charting and assessing the lactate levels over a period of 2 hours is more meaningful than a single value.
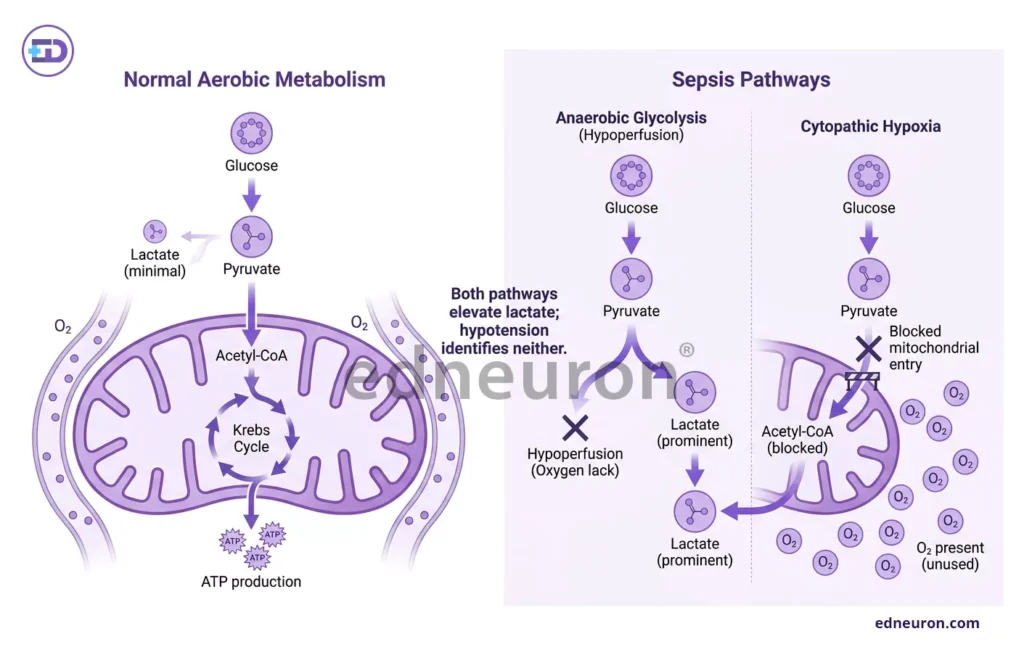
Fig 1: Difference in sepsis pathways from aerobic metabolism- anaerobic glycolysis and cytopathic hypoxia lead to increased lactate.
- The 2021 Surviving Sepsis Campaign endorses both capillary refill time and lactate marker as complementary perfusion targets. However, each has limitations:
- Lactate could be elevated in etiologies other than sepsis, including liver failure, metformin use, and adrenergic stress.
- Capillary refill time is subjective and examiner-dependent.
Neither can be, and should not be, interpreted in isolation.
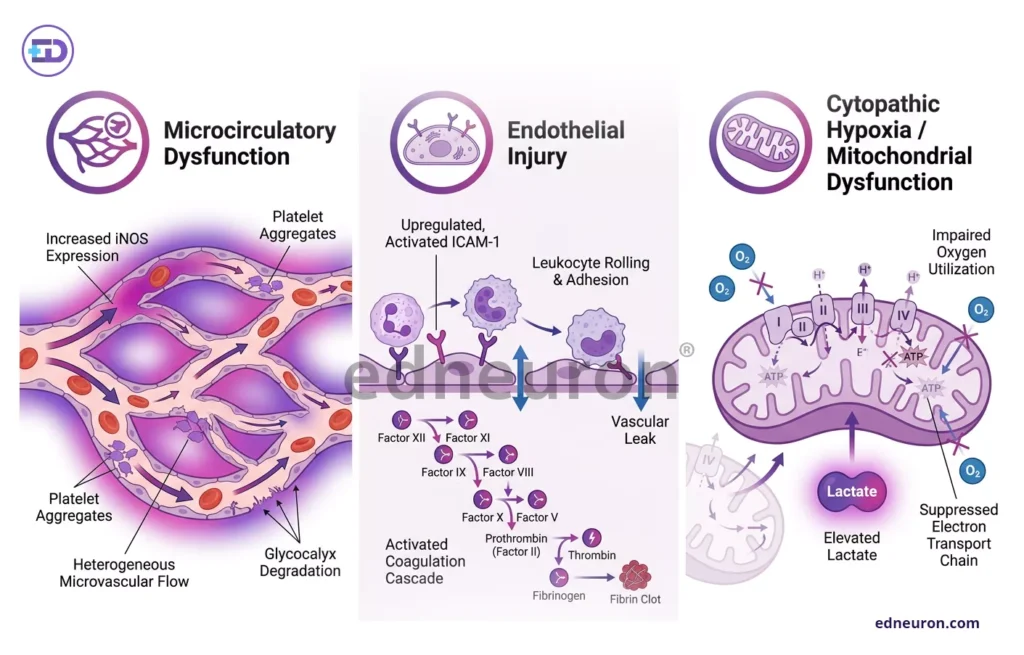
Fig 2: Pathophysiology involves the triad- microcirculatory dysfunction, endothelial injury and cytopathic hypoxia.
Clinical Consequences of Misclassification
The clinical cost of misclassifying a normotensive septic patient as ‘stable’ is measurable and significant. A 2024 meta-analysis by Tang F et al. confirmed that even a 1-hour delay in antibiotic administration worsens hospital sepsis mortality, and under-triage based on normal blood pressure is among the most common reasons for such delays in emergency settings. When such a normotensive patient with cryptic sepsis is held back for observation rather than being treated, the window of opportunity for rescue is quietly closing. The Sepsis-3 consensus definitions represent a conceptual shift in how our field understands this severity. The formal definition of septic shock is revised to categorize it not only as vasopressor-refractory hypotension but also as a lactate level exceeding 2 mmol/L, explicitly recognizing that hypotension alone is an incomplete phenotype. These frameworks and revisions refine thinking to conceptual insights- ‘Is the blood pressure low?’ to ‘Is perfusion adequate?’, allowing one to view shock as a subset of sepsis and not the sole entire picture. Normotension is a hemodynamic observation, not a marker of physiologic adequacy. A patient may maintain a normal MAP through compensatory mechanisms, even while their microcirculation is failing, and the clinician must acknowledge that compensation is finite and inadequate to sustain when the underlying problem remains uncorrected.
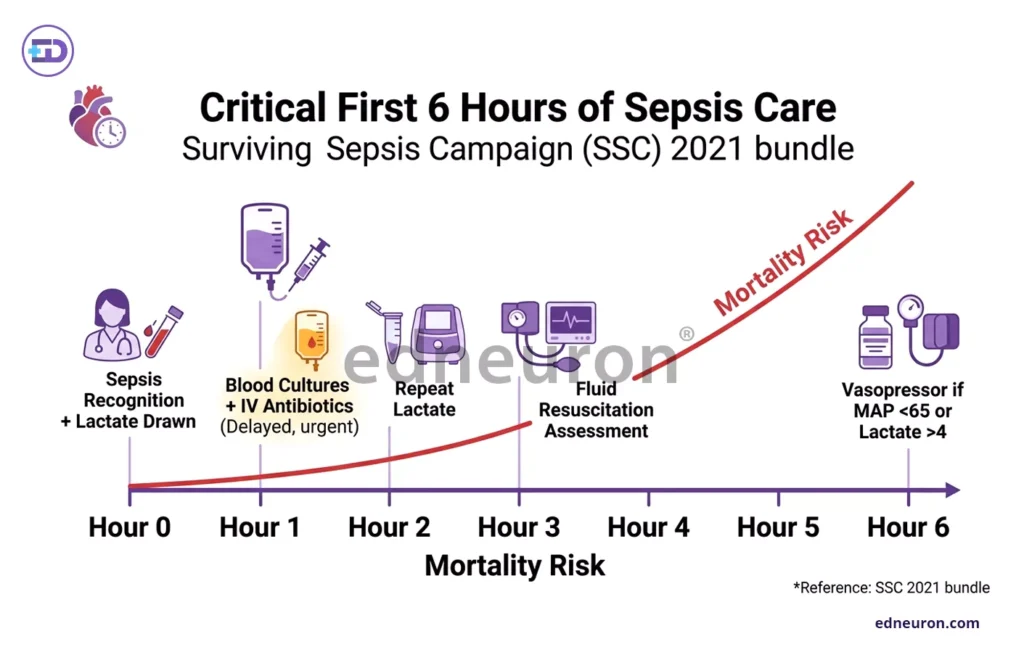
Fig 3: Prompt action is required to save the patient before the critical window of sepsis closes
Conclusion
From pressure to perfusion, from wait-and-watch to action, from reassurance to vigilance- thus becomes this indispensable mantra, and a clinician must be flexible to undergo dynamic re-orientation while managing. It is indeed undeniable that any delays in recognition translate directly into preventable deaths in these patients. Continuous monitoring, charting the trajectory, and prompt initiation of the sepsis bundle must not be contingent on the development of hypotension. In sepsis, the absence of hypotension is not reassurance, it is often nothing more than a delay in recognition.
References
- Puskarich MA, Trzeciak S, Shapiro NI et al.; Emergency Medicine Shock Research Network (EMSHOCKNET). Outcomes of patients undergoing early sepsis resuscitation for cryptic shock compared with overt shock. Resuscitation. 2011 Oct. PMID: 21752522.
- Marcos Miranda, Michelle Balarini, Daniella Caixeta, and Eliete Bouskela Microcirculatory dysfunction in sepsis: pathophysiology, clinical monitoring, and potential therapies
American Journal of Physiology-Heart and Circulatory Physiology 2016 311:1, H24-H35 10.1152/ajpheart.00034.2016 . - Mikkelsen ME, Miltiades AN, Gaieski DF et al. Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock. Crit Care Med. 2009 May.. PMID: 19325467.
- Dar, I. H. & None, M. S. (2025). Serum Lactate As a Prognostic Marker in Sepsis: A Prospective Study. Journal of Contemporary Clinical Practice, 11(9), 764-770.
- Tang F, Yuan H, Li X, Qiao L. Effect of delayed antibiotic use on mortality outcomes in patients with sepsis or septic shock: A systematic review and meta-analysis. Int Immunopharmacol. 2024 Mar. PMID: 38310764.
- Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi
