

Introduction
Even if one could draw very careful lines between various asphyxial deaths, it is imperative not to limit our thinking one-dimensionally. Although Stangulation and hanging in the realm of forensic science exhibit distinct conceptual mechanisms, one can also perhaps say the difference more often than not lies in agency too- one being an act of suicide, the other culpable homicide. Different mechanisms look very different in theory, but they converge at a single terminus- cerebral hypoxia via occlusion of cervical vessels. These convergences exist at high stakes, one that isn’t just academic but also medicolegal. Misclassification becomes an inverted verdict- one of homicide becomes a staged suicide, leading to the culprit’s immunity and a natural death reconstructed as intended violence. As Knight’s Forensic Pathology and successive guidelines affirm that accurate determination demands far more than just pattern recognition at the neck.
Comparative Pathophysiology and Autopsy Findings
Hanging produces pressure abrasion due to body weight, either wholly or partially; in rare cases, asystole may result from carotid compression, thereby triggering vagal activation and precipitating cardiac arrest. In contrast, strangulation outlines local compression, ischemic injuries, and tracheal rupture over a shorter anatomical arc with immense force, putatively insinuating a lateral or force upended from behind. The most traditional and apparent classification, which perhaps provides clearer distinctions, is ligature mark morphology. In hanging, the ligature furrow is oblique ascending to the highest point of suspension, the knot (commonly subaural followed by occipital), non-continuous with parchmentised edges, pale fascia below and mostly above the level of the thyroid.
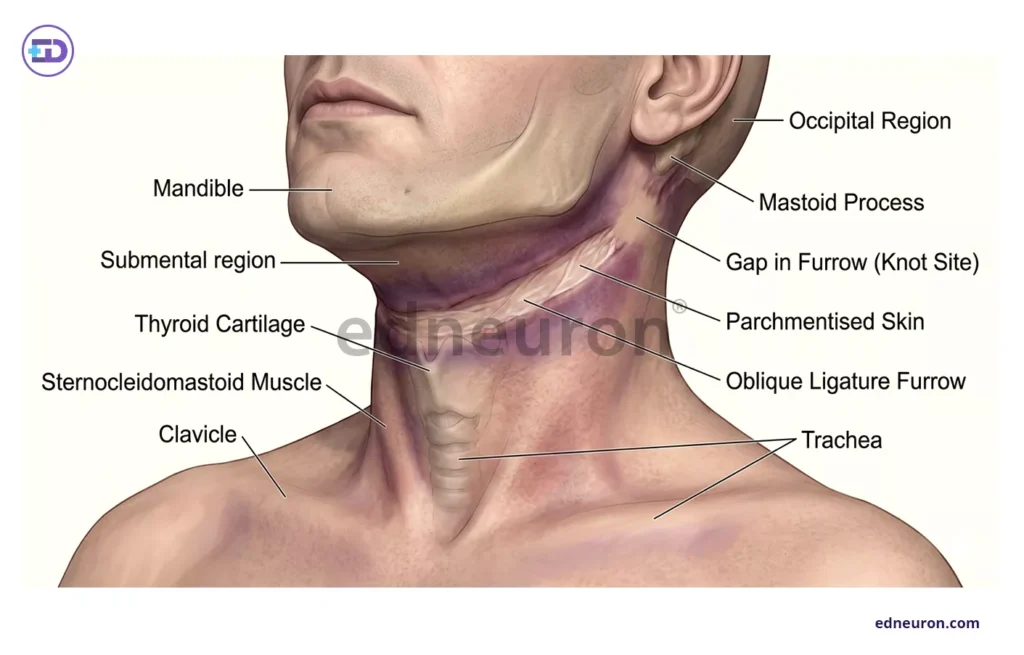
Fig 1: Ligature morphology in the case of hanging.
In strangulation, we find horizontal or circular ligature marks singly or doubly wound, with dark bruised hemorrhagic margins encircling completely, at or below the level of the thyroid, and multiple signs of struggle and defense injuries. Yet this distinction, while instructive, is neither invariably consistent nor sufficient. Incomplete suspensions, repositioning of ligatures, and post-mortem decomposition do waver in confident classification. The hyoid bone and thyroid cartilage occupy the central contentious place in this differential.
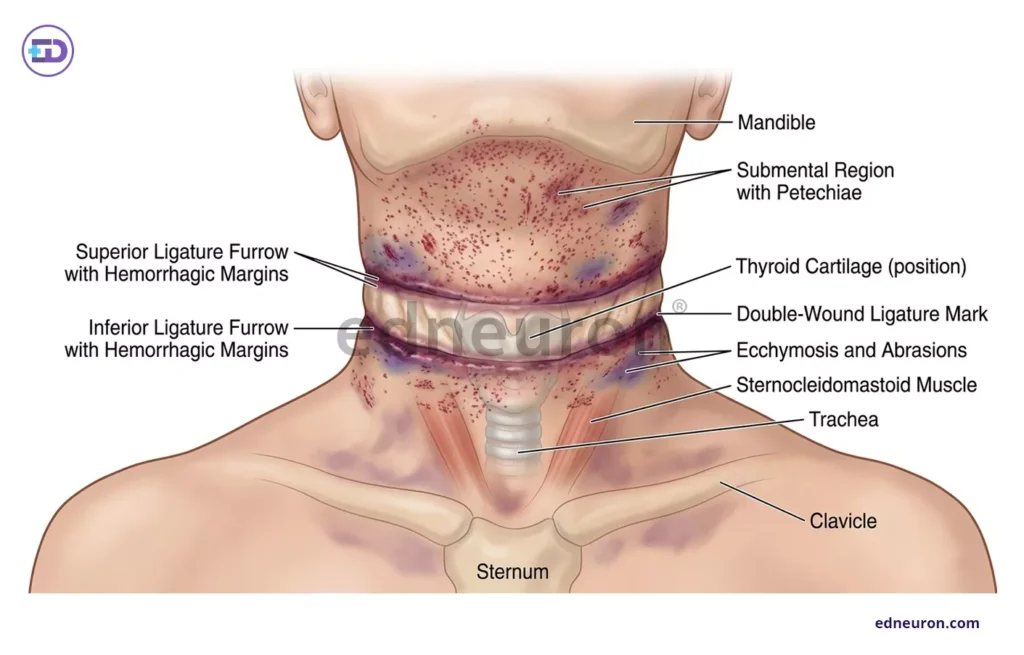
Fig 2: Ligature morphology in the case of strangulation.
Fracture of the hyoid for a long time is treated as a presumptive indicator of homicidal strangulation, but the fact that fracture rates are proportional to increasing age as the bone ossifies, its rarity in younger victims is unreliable as exculpatory evidence, and fracture patterns in hanging are neither rare nor negligible. The classical findings of asphyxia, i.e., petechial hemorrhages: conjunctival, scleral, and facial, face congestion, cyanosis, and tongue protrusion are similarly contested. Petechiae are more common in hanging cases than in non-hanging cases, but their presence in non-hanging cases reduces their credibility as an independent diagnosis. Facial congestion and cyanosis result from impaired venous return and may not be exclusive to hanging but also other asphyxial deaths. making them unreliable for differentiation. Tongue protrusion, again commonly observed in hanging, may be a sign of alleviating rigor mortis and relaxation. This underscores the caprice of relying on a single sign in isolation in a medicolegal case.
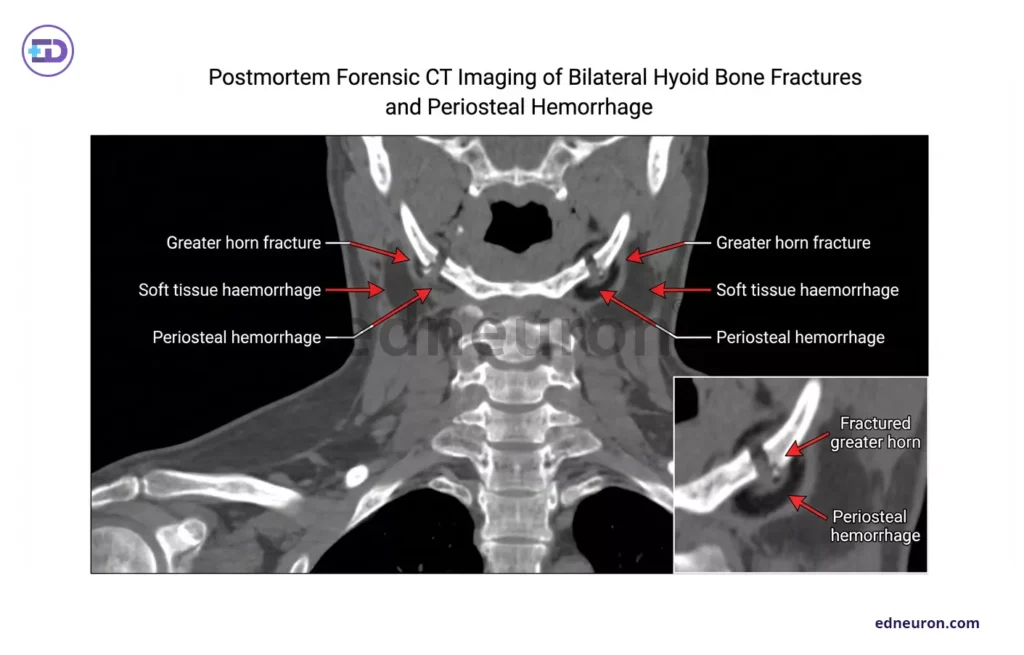
Fig 3: CT findings- fracture of greater horns of hyoid.
Advances in Forensic Diagnostics
New advances in technology address these very gaps in forensic science, though with some skepticism. Undeniably, postmortem CT and MRI have demonstrated value in visualizing deep cervical soft-tissue injury in high resolution with hyoid fracture patterns, soft tissue injuries, and subcutaneous hemorrhage distribution, without the distortion that dissection causes, as corroborated by Cianci V et al., 2024.
Moreover, with immunohistochemical adjuncts, a more robust assessment of antemortem and postmortem injury can be achieved.

Table 1: Ref- A Comparative Forensic Assessment of Hanging and Strangulation with Reference to Autopsy Findings. 2026.
These biomarkers represent the distinct biomolecular and cellular changes occurring in hanging vs strangulation. Strangulation, being intense localized stress and ischemia, causes intense activation of heat shock proteins (HSP27/70/90), consequently leading to Ubiquitin proteasome activation. The local ischemia-induced apoptosis also augurs the caspase cascade. Hanging, which reflects more pronounced global hypoxia, has patchy or incontiguous expression of HSP, but marked VEGF and HIF-1.
Ethical and Medico-Legal Implications
The medico-legal implications of misclassification extend beyond just the certification of death. Any error in incorrectly certifying suicide forecloses criminal investigation, denies families the truth of their
Bereavement and insurance distort public health data and permit perpetrators’ impunity. Similarly, a false misclassification would cost an innocent life and warp judicial proceedings. This responsibility demands that interpretation mandates scene reconstruction, circumstantial coherence, and explicit acknowledgment of diagnostic uncertainty.
Conclusion
No single autopsy finding carries sufficient discriminatory weight or empirical objectivity to resolve the hanging-strangulation in isolation. The forensic determination emerges, when it can, from a synthesis of the scene. Where uncertainty persists even after complete synthesis of the scene from circumstantial evidence, witness, and forensic evidence, it must be stated explicitly rather than dissolved just for diagnostic convenience. Forensic pathology serves justice most faithfully not when it delivers certainty without foundation, but when it maps the boundaries of what the evidence genuinely permits, and resists the pressure to concoct beyond it.
References
- A Comparative Forensic Assessment of Hanging and Strangulation with Reference to Autopsy Findings. 2026.
- Saukko P, Knight B. Knight’s Forensic Pathology. 4th ed. CRC Press; 2016.
- A Scoping Review of Strangulation and Hanging. 2025.
- Cianci V, Mondello C, Cracò A et al. Hyoid Bone Fracture Pattern Assessment in the Forensic Field: The Importance of Post Mortem Radiological Imaging. Diagnostics (Basel). 2024 Mar PMID: 38611588.
- Zhang, S., Nosaka, M., Kuninaka, Y. et al. (2023). Forensic application of epidermal expression of HSP27 and HSP70 for the determination of wound vitality in human compressed neck skin. Scientific Reports, 13, 33799.
- Zhang et al (2022). Forensic application of epidermal ubiquitin expression to the determination of wound vitality in human compressed neck skin. Frontiers in Medicine, 9, 867365.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi

