Introduction
Trisomy 21 poses a unique challenge for clinicians: how can we distinguish harmless changes caused by extra genes from early signs of cancer?
When caring for children with Down Syndrome, clinicians often see ongoing lab changes like macrocytosis, leukopenia, and neonatal cytopenias. In most patients, these would prompt further testing, but for children with DS, they are often normal. This creates a challenge: doctors must decide when these changes are harmless and when they might signal the start of leukemia.
The Ubiquity of Macrocytosis: A Metabolic or Dosage Epiphenomenon?
Macrocytosis is very common in children with Down Syndrome. Studies show that up to 60.4% have a high mean corpuscular volume (MCV), even in the absence of anemia, and because this is so common, it can make diagnosis a lot harder. Normally, macrocytosis points to nutritional problems or bone marrow issues, but in DS, it seems to be a natural part of having an extra chromosome.
One possible reason for this is that the cystathionine-β-synthase (CBS) gene is present in three copies on chromosome 21. This extra gene may alter how the body processes folate, leading to macrocytosis not due to nutritional deficiency. For doctors, this means macrocytosis can hide iron deficiency or cause them to stop looking for other problems too soon. A normal hemoglobin level in a child with DS and macrocytosis may indicate mild anemia, so careful testing for iron, B12, and folate is important.
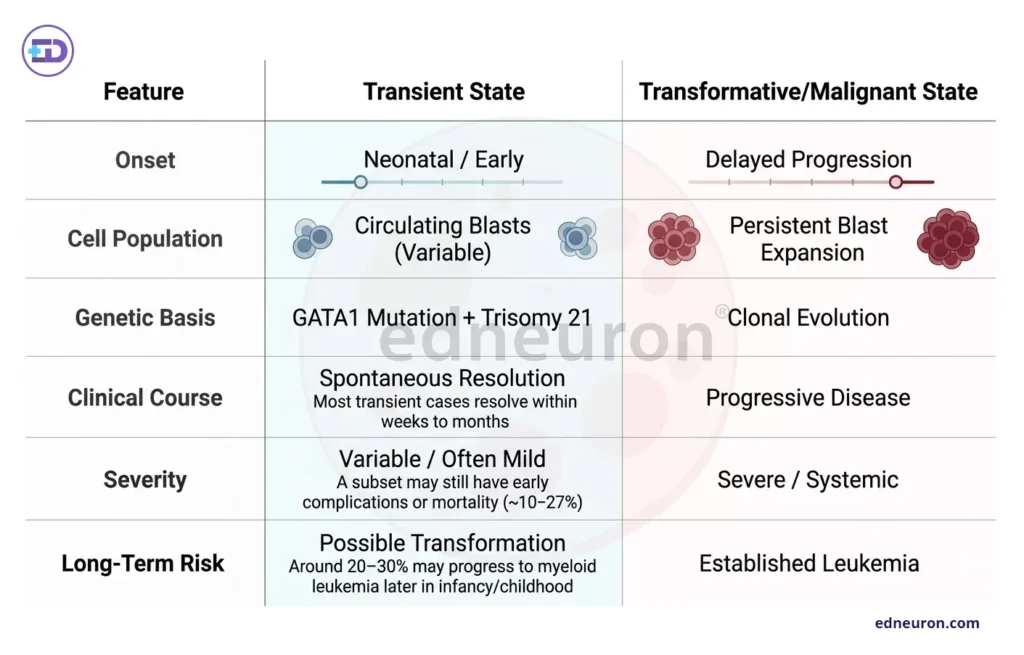
Fig 1: Transient and Malignant Hematologic Changes in Neonates: Onset, Characteristics, and Prognosis.
The Neonatal Hematological Storm: Transience vs. Transformation
The neonatal period in DS is characterized by a dramatic, often chaotic, hematological profile. Recent retrospective analyses show that over 50% of DS newborns admitted to intensive care exhibit thrombocytopenia. While these cytopenias are often transient—resolving spontaneously within the first two to three weeks of life—they exist in the shadow of Transient Abnormal Myelopoiesis (TAM).
About 10% of newborns with DS develop TAM, which shows up as abnormal cells in the blood that look like leukemia. The problem is that many normal newborn blood changes, like mild increases in certain cells, can look similar to TAM. Most TAM cases get better on their own, but about 20% of these babies later develop acute megakaryoblastic leukemia (AMKL). Because of this, doctors need to monitor these children closely, even if their blood counts seem to return to normal after two weeks. The genetic changes, often involving GATA1 mutations, can increase the risk of cancer in ways that regular blood tests might not catch early.
Lineage Deviations and Immunologic Fragility
Children with DS also often have ongoing changes in their white blood cells, like low white cell counts (10.7%) and low lymphocyte counts (23.5%). These changes are important because they may help explain why DS patients have high rates of serious infections, such as the 50% sepsis rate seen in newborns. Many of these children also have breathing problems and heart defects, which can make their health issues worse when combined with immune system weaknesses.
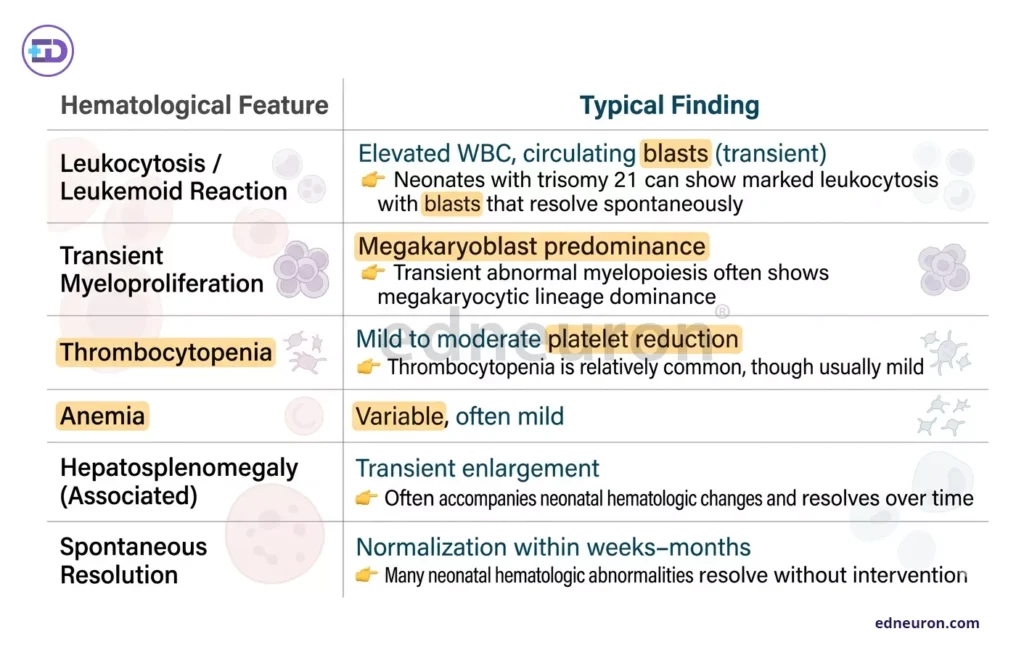
Fig 2: Summary of non-malignant hematological alterations commonly observed in children with Down syndrome, highlighting characteristic features and their typical clinical findings.
Therapeutic Efficacy and Functional Consequences
The reliance on standard pediatric reference ranges often leads to misinterpretation of DS blood counts. Because pediatric values vary significantly by age and sex, the absence of DS-specific reference intervals means clinicians must often rely on longitudinal trends within a single patient rather than static thresholds. Furthermore, the evolution of these phenotypes—such as the neonatal shift from thrombocytopenia to later-childhood thrombocytosis (seen in 10.2% of older cohorts)- suggests that the marrow environment in Trisomy 21 is in a state of constant, age-dependent flux.
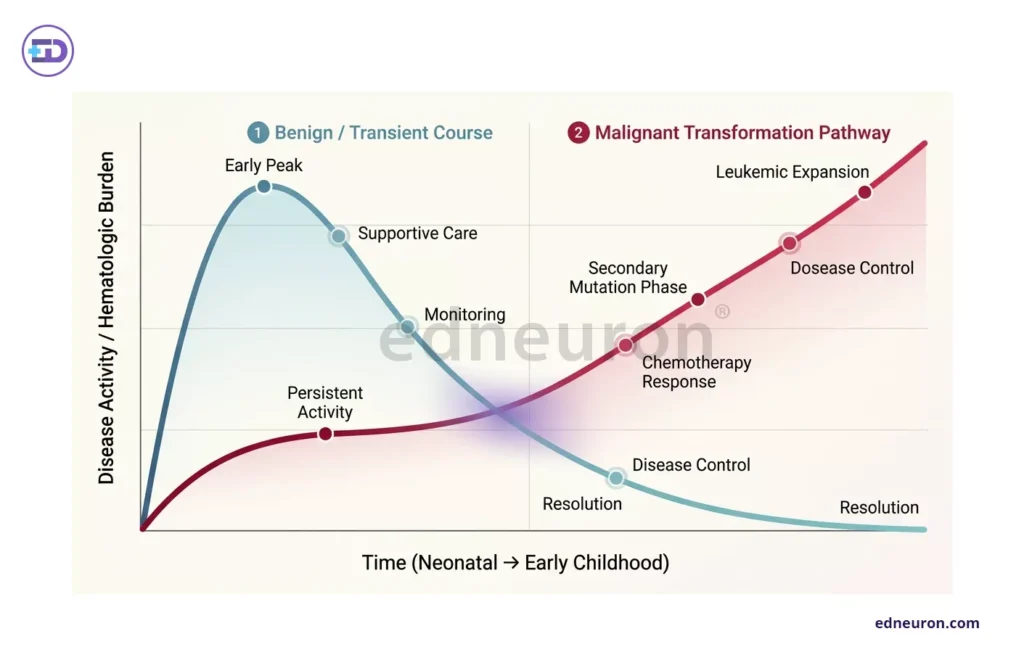
Fig 3: A comparative graph illustrating that while most cases of Transient Abnormal Myelopoiesis (TAM) in neonates with Down syndrome resolve spontaneously, 20–30% of these cases progress to Acute Megakaryoblastic Leukemia (AMKL) in early childhood due to additional mutations.
Conclusion
Simply listing blood changes in Down Syndrome does not capture the complexity of the clinical work. Doctors need to see these findings as part of a unique pattern, where harmless differences are common, but the risk of cancer is higher than usual. The aim is not to make the blood counts look normal, but to understand them as the patient’s own baseline and to keep monitoring them over time.
References
- Tsou, P. Y., Wang, Y. H., & Tapia, I. E. (2025). Inpatient outcomes in children with Down syndrome using the Kids’ Inpatient Database. BMC Pediatrics, 25, Article 5899.
- Rodríguez, A. O., et al. (2025). Factors associated with breastfeeding in children with Down syndrome. BMC Pediatrics, 24, Article 5363.
- García de la Puente, S., et al. (2022). Blood cytology in children with Down syndrome. BMC Pediatrics, 22, Article 3450.
- Asim, A., Kumar, A., Muthuswamy, S., Jain, S., & Agarwal, S. (2015). Down syndrome: An insight of the disease. Journal of Biomedical Science, 22(1), 41.
- (2024). Sleep study patterns in children with Down syndrome. Pediatrics Open Science.
- Şimşek, H., et al. (2025). Clinical profile and outcomes of newborns with Down syndrome: A single-center experience. Journal of Pediatric Academy.
- Journal of Down Syndrome & Chromosome Abnormalities. (n.d.). Down syndrome research articles (open access collection).

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India