

Introduction
Acute Respiratory Distress Syndrome (ARDS) represents a profound failure of the alveolar–capillary unit, where structural disruption, inflammatory injury, and vascular dysregulation converge to impair oxygen transfer. The defining clinical feature—refractory hypoxemia—reflects not a lack of delivered oxygen, but a failure of that oxygen to access and equilibrate with pulmonary blood flow.
Pathophysiological Basis of Gas Exchange Failure
ARDS is fundamentally driven by diffuse alveolar damage, which increases the permeability of the alveolar–capillary barrier. Protein-rich edema accumulates in the alveolar space, while infiltration by inflammatory cells and cytokine release perpetuate epithelial and endothelial injury. The resulting loss of barrier integrity causes both ventilation failure, due to alveolar filling and collapse, and perfusion dysregulation, due to endothelial dysfunction and microvascular injury. This dual impairment disrupts the essential coupling of ventilation and perfusion, leading to conditions in which even high concentrations of inspired oxygen cannot effectively participate in gas exchange.
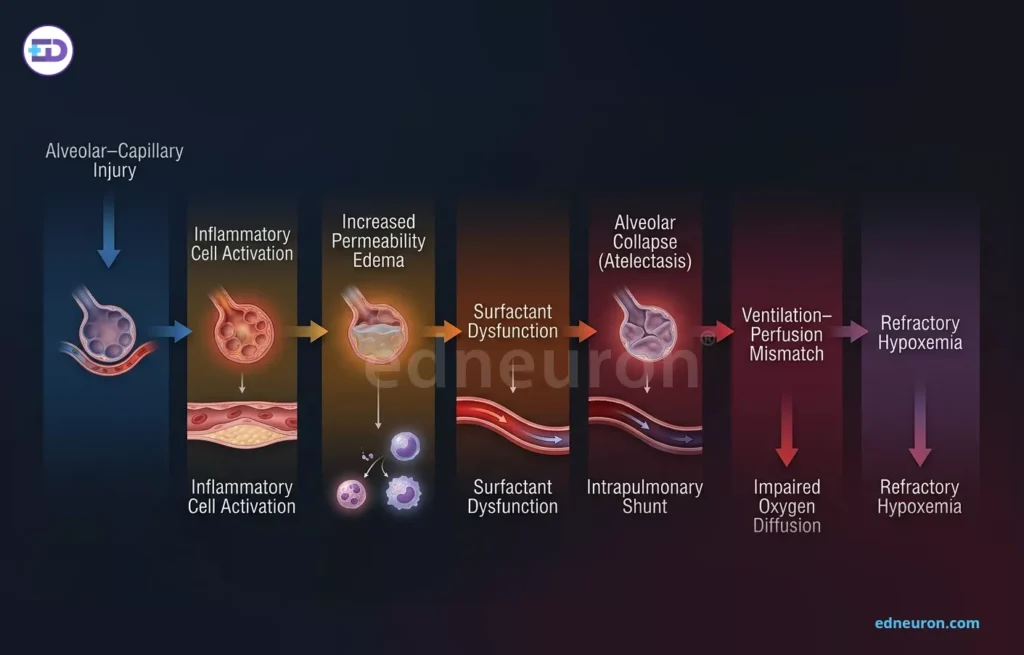
Fig 1: Sequential pathogenesis of ARDS from alveolar–capillary injury to inflammation, edema, surfactant dysfunction, atelectasis, V/Q mismatch, and refractory hypoxemia.
The Dominance of True Intrapulmonary Shunt
The principal mechanism underlying oxygen failure in ARDS is true intrapulmonary shunting, wherein pulmonary capillary blood traverses non-ventilated alveoli—whether fluid-filled, collapsed, or consolidated.
Clinical Data: In severe ARDS, shunt fractions (Qs/Qt) frequently exceed 30–50%, compared to less than 5% in healthy lungs.
The Plateau Effect: Because shunted blood bypasses ventilated alveoli entirely, increasing the fraction of inspired oxygen (FiO₂) up to 1.0 produces minimal improvement in arterial oxygen tension (PaO₂). Hemoglobin in ventilated units is already near maximal saturation at lower FiO₂ levels, and additional oxygen contributes only marginally via dissolved plasma oxygen, insufficient to offset the impact of large-volume shunting.
V/Q Heterogeneity and the “Baby Lung” Concept
ARDS is characterized by extreme spatial heterogeneity, in which only a fraction of the lung, the so-called “baby lung,” remains aerated and functionally available for gas exchange.
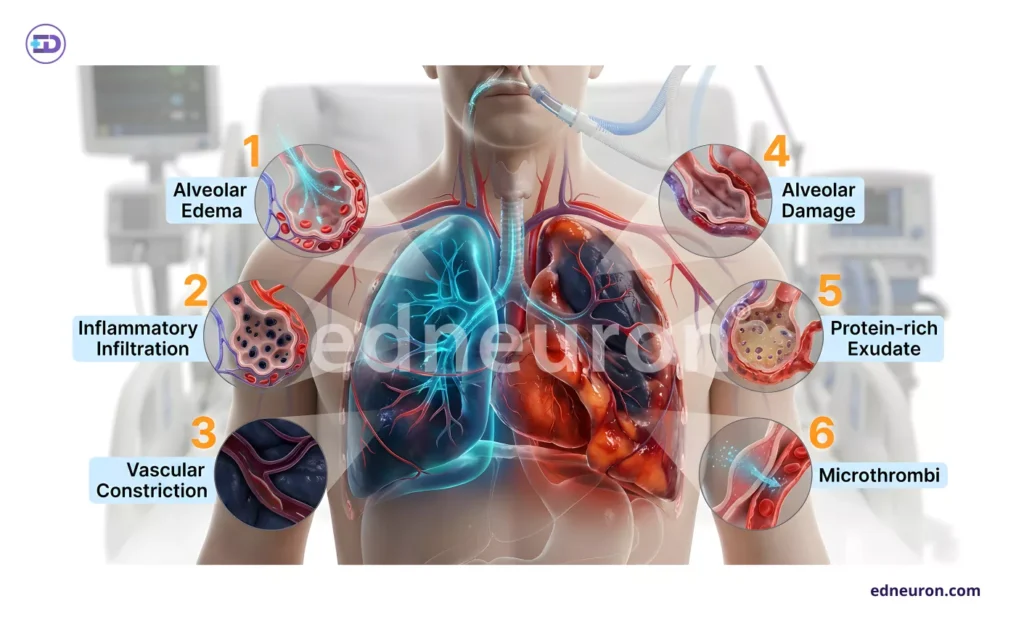
Fig 2: Pathophysiological cascade of ARDS illustrating alveolar edema, inflammatory infiltration, vascular constriction, alveolar damage, protein-rich exudation, and microthrombi formation.
HPV Dysfunction: Normally, hypoxic pulmonary vasoconstriction (HPV) diverts blood flow away from poorly ventilated regions. In ARDS, inflammatory mediators such as nitric oxide and prostacyclins blunt this compensatory mechanism, allowing continued perfusion of non-aerated units and exacerbating shunt physiology.
Surfactant Failure: Injury to type II pneumocytes leads to surfactant depletion, increasing surface tension and promoting alveolar instability. The result is repetitive collapse and reopening (atelectrauma), further reducing the proportion of lung available for effective ventilation.
Microvascular Pathology and Diffusion Barriers
The pulmonary vasculature is not merely a passive conduit but an active site of injury in ARDS.
Microthrombosis: Endothelial disruption activates coagulation pathways, leading to microthrombi formation. This contributes to increased physiological dead space and further distorts perfusion distribution.
Diffusion Limitation: Although secondary to shunt, diffusion impairment arises from thickened alveolar-capillary membranes due to interstitial edema and hyaline membrane formation. In high-flow states such as sepsis, shortened capillary transit time may further limit oxygen equilibration.
The Oxygen Paradox and Clinical Correlates
Excessive reliance on high FiO₂ can be counterproductive. Sustained exposure to FiO₂ levels above 0.6 promotes the generation of reactive oxygen species (ROS), exacerbating epithelial injury and impairing surfactant function, thereby perpetuating the cycle of lung damage.
Clinical Markers of Severity: Severe ARDS is defined by a PaO₂/FiO₂ ratio below 100.
Therapeutic Shift: Given that the primary defect lies in oxygen accessibility rather than availability, effective management emphasizes alveolar recruitment strategies, such as positive end-expiratory pressure (PEEP) and prone positioning, rather than indiscriminate increases in FiO₂.
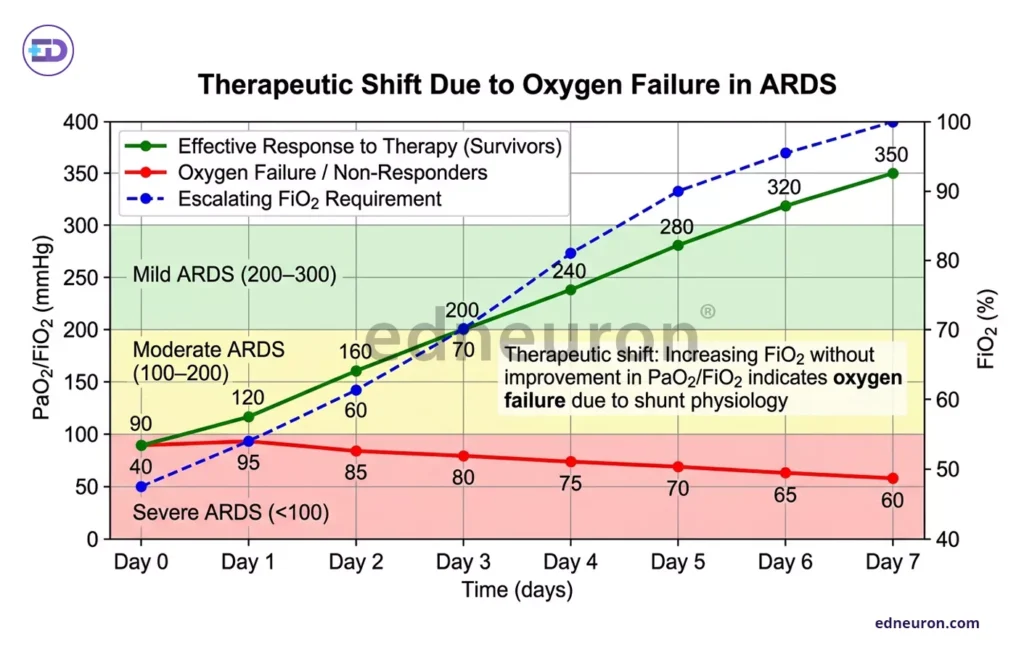
Fig 3: A comparative graph illustrating that while most cases of Transient Abnormal Myelopoiesis (TAM) in neonates with Down syndrome resolve spontaneously, 20–30% of these cases progress to Acute Megakaryoblastic Leukemia (AMKL) in early childhood due to additional mutations.
Conclusion
Refractory hypoxemia in ARDS is a manifestation of profound structural and functional disintegration of the lung, in which oxygen delivery is rendered ineffective by shunt physiology, ventilation–perfusion mismatch, and microvascular dysfunction. The failure of supplemental oxygen is therefore not paradoxical but expected within this altered physiological landscape. Clinical management must align with this reality, shifting focus from escalating oxygen concentrations to restoring alveolar participation and optimizing perfusion distribution. Only by addressing the inaccessibility of ventilated units can meaningful improvements in oxygenation be achieved.
References
- Ralston SH, Penman ID, Strachan MWJ, Hobson RP, editors. Davidson’s Principles and Practice of Medicine. 24th ed. Edinburgh: Elsevier; 2022.
- Thompson BT, Chambers RC, Liu KD. Acute respiratory distress syndrome. N Engl J Med. 2017;377(6):562–72.
- Harrison’s Principles of Internal Medicine. Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J, editors. 21st ed. New York: McGraw-Hill Education; 2022.
- Murray and Nadel’s Textbook of Respiratory Medicine. Broaddus VC, Mason RJ, Ernst JD, King TE Jr, Lazarus SC, Murray JF, Nadel JA, editors. 6th ed. Philadelphia: Elsevier Saunders; 2016.
- Chugh SN. Textbook of Medicine. 4th ed. New Delhi: Jaypee Brothers Medical Publishers; 2019.
- John J. Marini, Arthur S. Slutsky. Physiological basis of ventilatory support in acute lung injury. Am J Respir Crit Care Med. 1998;158(6):1839–46.
- Ohshimo S. Oxygen administration for patients with acute respiratory distress syndrome. J Intensive Care. 2021;9(1):17.
- Fujishima S. Pathophysiology and biomarkers of acute respiratory distress syndrome. J Intensive Care. 2014;2(1):32.
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–33.
- Fan E, Brodie D, Slutsky AS. Acute respiratory distress syndrome: advances in diagnosis and treatment. JAMA. 2018;319(7):698–710.
- Matthay MA, Zemans RL, Zimmerman GA, Arabi YM, Beitler JR, Mercat A, et al. Acute respiratory distress syndrome. Nat Rev Dis Primers. 2019;5(1):18.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



