

Introduction
Witnessing the paradigm shift to NCDs calls for ever-evolving changes in how we treat patients with DM type 2, personalizing therapy rather than resorting to metformin and sulfonylureas alone. Ever since the advent of GLP-1 receptor agonists and SGLT2 inhibitors, the management landscape has drastically changed. Despite the versatility of these options, most glucose-lowering therapies have not shown a significant effect on cardiovascular risk. In addition, contrary to the benefits, these have negative effects; for instance, notwithstanding the hypoglycemic effect of rosiglitazone, it has been shown (Singh S et al. 2007) to increase the risk of myocardial infarction (MI) by 42% and heart failure by 109%. Beyond glycemic control, studies show increased cardiovascular and renal protective benefits independent of lowering glucose levels. So the main question isn’t whether there is a clear-cut winner, the one true superior class? Rather, which one to use when? The answers are more often than not right in the front seat.
How do these Putative Drugs Bring About Such Crucial Benefits in the Course of a Disease So Heavily Laced with Micro and Macrovascular Changes?
GLP-1 RAs: the glutides, including semaglutide and liraglutide, mimic the incretins in our gut, promoting insulin secretion and inhibiting glucagon, with additional effects such as delayed gastric emptying and central promotion of satiety centers, leading to reduced food intake. Interestingly, they also prevent macrophage adhesion and platelet activity, thereby establishing themselves as invaluable in preventing stroke and thromboembolism. Studies have shown they can lead to an average decrease in HbA1C of 0.9–2.2% and a weight reduction of 1.3-8.65 kg.

Fig 1: GLP1 agonist works on the pancreas to decrease glucagon and increase insulin, reduces inflammatory markers, and helps in glycemic control. SGLT-2 inhibitors work on the kidneys to block glucose and sodium co-transporter thereby causing glycosuria.
SGLT2 inhibitors: empagliflozin, dapagliflozin, prevent renal glucose reabsorption and, intuitively, as we all understand, promote glycosuria-osmotic diuresis- the major driving mechanism to reduce preload and afterload in patients with heart failure. Apparently, the secondary absorption of glucose to compensate for the lack of insulin lowers HbA1C levels by approximately 0.5–1.0% with a more modest 2–4% weight loss.
Understandably so, because of the distinct mechanism in which the two bring about their effect, we can easily categorize that GLP 1RA- primarily reducing the atherosclerotic events- proves more beneficial in cases of stroke and myocardial infarction. On the other hand, SGLT-2 Inhibitors have dramatic effects in patients with heart failure and chronic kidney disease (CKD). (Rhee JJ et al. 2024) documents:

Fig 2 : Comparative statistical chart of events in patients using the newer drugs.
When to Prefer One Over Other?
Based on the current ADA Guidelines– Remember, risk Stratification is a must to optimize benefits to fit the patient profile. SGLT2 inhibitors are the preferred choice in patients with established heart failure or CKD (eGFR ≥20 mL/min/1.73 m2). At the same time, GLP-1 RAs are preferred where established atherosclerotic cardiovascular disease (ASCVD) or high stroke risk becomes our main concern. Diabetes Canada 2024 takes it even further as an anti-obesity drug where weight loss is our primary goal, especially in NAFLD, obstructive sleep apnoea, and metabolic syndrome.
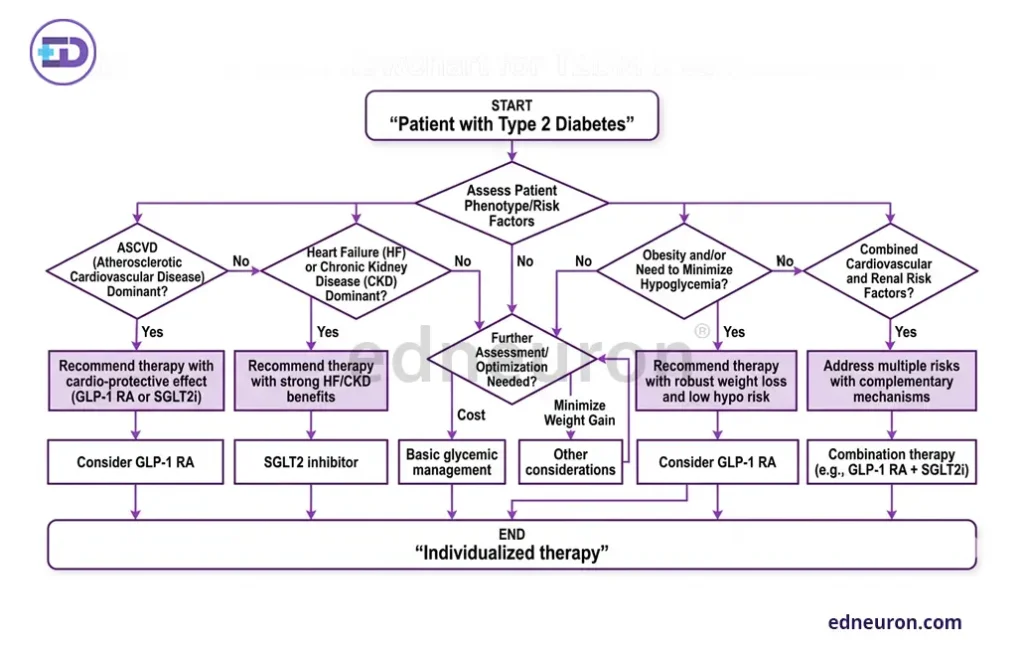
Fig 3 : Risk Stratification workflow.
Can the Combination Provide Indomitable Synergism? YES Indeed!
In patients with multiple comorbidities and moderate-to-high renal risks, this proves to be just the potion to maximize these evidence-based advantages. However, one must never forget that practical prescribing requires more than matching drugs to diagnosis. How much a patient can tolerate must be taken into account: GLP-1 RAs can cause distressing nausea and vomiting, and SGLT2 inhibitors carry a risk of genitourinary infections and require adequate patient hydration. What one might deem empathetically prudent for patients’ socioeconomic fitness is that drug cost and injectable routes of administration become perhaps this strong noose limiting patient compliance and their wider implementation. Ultimately, the choice is less about which drug is better and more about identifying which organ is most at risk, which comorbidity dominates the clinical picture, and what the patient is most likely to tolerate and sustain long-term.
References
- Rolek B, Haber M, Gajewska M et al. SGLT2 Inhibitors vs. GLP-1 Agonists to Treat the Heart, the Kidneys and the Brain. J Cardiovasc Dev Dis. 2023 Jul PMID: 37623335.
- Singh S, Loke YK, Furberg CD. Long-term risk of cardiovascular events with rosiglitazone: a meta-analysis. JAMA. 2007 Sep PMID: 17848653.
- Brown E, Heerspink HJL, Cuthbertson DJ et al. SGLT2 inhibitors and GLP-1 receptor agonists: established and emerging indications. Lancet. 2021 Jul PMID: 34216571.
- Helmstädter J, Keppeler K, Küster L et al. Glucagon-like peptide-1 (GLP-1) receptor agonists and their cardiovascular benefits-The role of the GLP-1 receptor. Br J Pharmacol. 2022 Feb PMID: 33764504.
- Rhee JJ, Han J, Montez-Rath ME, Chertow GM. Comparative effectiveness of sodium-glucose cotransporter-2 inhibitors versus glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes and mild/moderate chronic kidney disease. Diabetes Obes Metab. 2024 Apr PMID: 38186297.
- ElSayed NA, Aleppo G, Aroda VR et al.,on behalf of the American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes-2023. Diabetes Care. 2023 Jan PMID: 36507650.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



