

Introduction
Refeeding Syndrome (RFS) can almost be viewed as a metabolic insurgency to an adaptive starved state that follows, although well-intentioned but imprudent reinstatement of nutrition (enterally or parenterally) in chronically malnourished people, eating disorders, depression, renal failure, malabsorptive conditions, previous bariatric surgery, post-surgical patients, and alcohol abuse. Historically, we can date its early documentation to WW2, when survivors of wartime sieges were granted sudden access to food. Almost 1/5th of starved Japanese prisoners died suddenly when provided with nutritional supplementation. One can justifiably ponder why, despite the clinical vehemence, RFS remains substantially underdiagnosed. This can be attributed to a mosaic of inconsistencies, non-standardized definitions, inappropriate treatment, and a lack of awareness among clinicians. For the practicing physician, RFS represents an instructive model of iatrogenic harm: its prevention demands systematic risk stratification before feeding is initiated.
Pathophysiology
During prolonged starvation, the body, under extreme stress, depletes glycogen stores within 24–72 hours and shifts to catabolizing fat and protein as primary energy substrates. So as the body switches from an insulin-sufficient, energy-assimilating phase to an insulin-depleted, utilizing phase, there is decreased glycolysis and increased gluconeogenesis. However, since our bodies’ priority, more or less, remains sustaining brain activity, the rest aims to prevent protein and muscle breakdown, shifting from ketone bodies to fatty acid consumption, sparing the former for the brain. Intracellular reservoirs of cations, particularly phosphate, magnesium, and potassium, are depleted, yet serum concentrations may remain deceptively normal due to transcellular redistribution and reduced renal excretion. Hell unleashes upon early reinstatement of a high-carbohydrate diet, leading to a drastic surge in insulin levels. Insulin via the sodium-potassium symporter pushes potassium into the cells along with magnesium, phosphorus, and thiamine. The severe depletion of thiamine, a cofactor in enzymatic reactions, can expose the patient to Wernicke encephalopathy (ophthalmoplegia, global confusion, and ataxia) and Korsakoff syndrome if not corrected. Simultaneously, insulin also promotes renal sodium and water retention, predisposing to fluid overload.
Hypophosphatemia is the biochemical hallmark of this transition. In a well-designed prospective cohort study by Marik PE et al., 34% of patients experienced hypophosphatemia soon after feeding was started (mean standard deviation 1.9 ± 1.1 days).
Phosphate, the most crucial ingredient of ATP synthesis, 2,3-DPG production, and intracellular signaling, its precipitous decline impairs oxygen delivery, reduces myocardial contractility, and disrupts neuromuscular function. This menagerie of metabolic havoc leading to multiorgan dysfunction encompassing cardiopulmonary, neurological, hematological, and urinary symptoms comes under RFS.
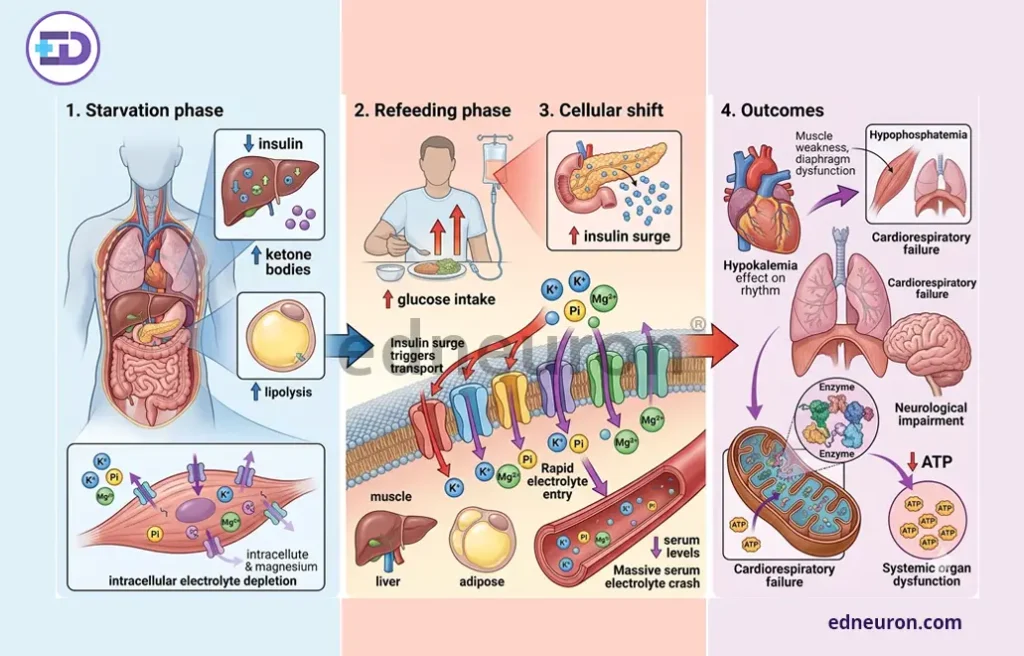
Fig 1 : Sudden refeeding phase results in an insulin spike, causing hypophosphatemia, hypokalemia, and systemic organ dysfunction.
Clinical Features and Risk Stratification
Symptoms cascade like a downpour within 72 hours of initiating nutrition and may have a rapid onset.
Cardiac arrhythmias due to hypokalemia, fluid overload leading to congestive cardiopulmonary failure, low ATP contributing to skeletal muscle weakness, rhabdomyolysis, seizures, delirium, and hemolytic anemia are all recognized complications.
The National Institute for Health and Care Excellence (NICE) guidelines elucidate risk stratification based on criteria:
- Body mass index below 16 kg/m2.
- Weight loss exceeding 15% over three to six months.
- Minimal or no nutritional intake for more than ten consecutive days.
- Low pre-feeding levels of serum potassium, phosphate, or magnesium.
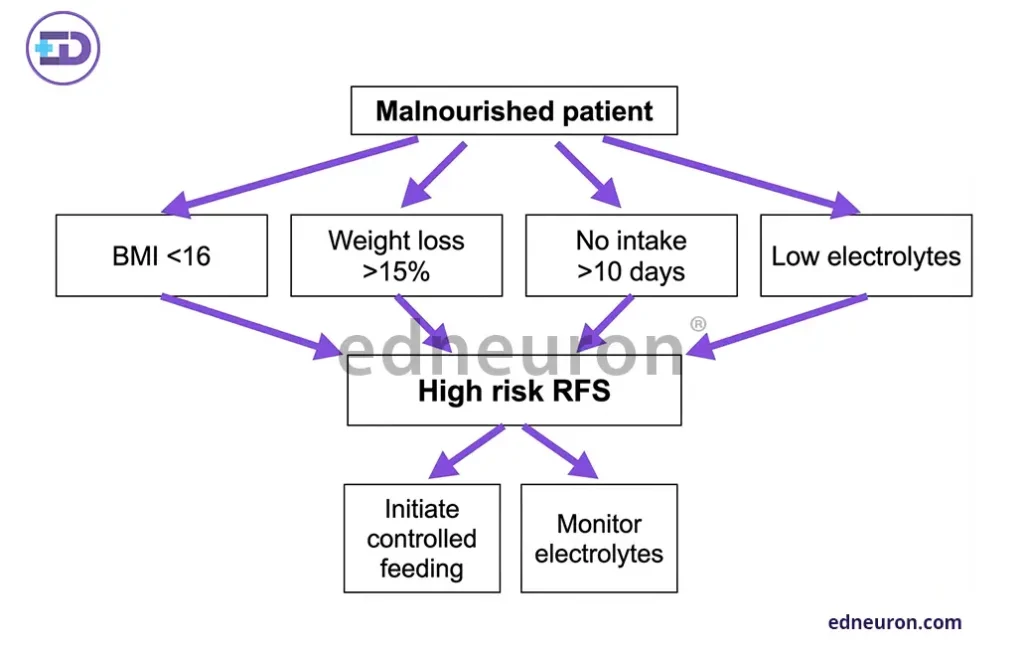
Fig 2 : Various parameters for risk stratification.
Management and Prevention
Identifying patients at high risk of RFS is pivotal to management. In the pediatric population, extra caution is warranted, as undernutrition and overfeeding are both deleterious. Moreover, nutritional support should be initiated at no more than 5–10 kcal/kg/day, increasing gradually over four to seven days to allow room for metabolic readaptation. However, one must never forget that instituting treatment will yield the most benefit when corroborated with the clinical context, as evidenced by a more recent study by Mosuka EM et al. (2023 in adolescent patients with anorexia nervosa), where higher-calorie refeeding protocols have demonstrated comparable safety with superior outcomes in terms of weight restoration and hospital duration, underscoring the need to calibrate according to circumstance.
Electrolyte replacement is paramount. Phosphate, potassium, and magnesium should be corrected proactively and monitored closely, ideally daily for the first week. Thiamine supplementation (at least 200–300 mg intravenously before any glucose administration) is mandatory in patients with suspected deficiency or alcohol-use disorder. Fluid balance must be monitored carefully to avoid precipitating pulmonary edema in the context of insulin-mediated sodium retention. Nutritional support teams, where available, have demonstrated benefit in reducing RFS-related complications through structured monitoring protocols and interprofessional coordination.

Fig 3 : Stepwise treatment protocol emphasizing structured and phased escalation to feeding in chronically ill patients.
Conclusion
RFS therapeutic management, thus, if instituted without a deep conceptual grasp and mechanistic understanding, can precipitate the very harm it seeks to prevent. Therefore, risk stratification using NICE guidelines, a slow phasing nutrient escalation, robust electrolyte surveillance, and thiamine management are the pillars of safe nutritional rehabilitation. This, undoubtedly, if properly instituted, can greatly reduce morbidity and mortality.
References
- Persaud-Sharma D, Saha S, Trippensee AW. Refeeding Syndrome. [Updated 2022 Nov 7]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2026 Jan.
- SCHNITKER MA, MATTMAN PE, BLISS TL. A clinical study of malnutrition in Japanese prisoners of war. Ann Intern Med. 1951 Jul;35(1):69-96. PMID: 14847450.
- Mehanna HM, Moledina J, Travis J. Refeeding syndrome: what it is, and how to prevent and treat it. BMJ. 2008 Jun 28;336(7659):1495-8. PMID: 18583681.
- Marik PE, Bedigian MK. Refeeding hypophosphatemia in critically ill patients in an intensive care unit. A prospective study. Arch Surg. 1996 Oct; PMID: 8857900.
- National Institute for Health and Care Excellence (NICE). Nutrition support for adults: oral nutrition support, enteral tube feeding, and parenteral nutrition. Clinical Guideline CG32. London: NICE; 2006.
- Mosuka EM, Murugan A, Thakral A E et al. Clinical Outcomes of Refeeding Syndrome: A Systematic Review of High vs. Low-Calorie Diets for the Treatment of Anorexia Nervosa and Related Eating Disorders in Children and Adolescents. Cureus. 2023 May PMID: 37351245.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



