

Introduction
Traditionally, the success of abdominal hernia repair (AHR) has been judged by recurrence and complication rates. Yet, with recurrence rates still as high as 45% after five years, surgeons are now focusing more on restoring abdominal wall function and reducing long-term complications. A key part of this shift is the debate over mesh fixation methods: trans-fascial sutures (TS) versus newer options such as tissue adhesives (TA) or self-fixating meshes. As the field moves toward more functional repairs, how the mesh is fixed is becoming just as important as the type of mesh used.
The Biomechanical Cost of Mechanical Anchoring
Traditional mesh fixation typically relies on penetrating devices, such as sutures, staples, or tacks. While these provide robust initial mechanical stability, they are frequently associated with “penetrating injuries” that may lead to nerve entrapment and ischemia. Biomechanical investigations using dynamic cine-MRI have demonstrated that the abdominal wall behaves as a sophisticated, dynamic unit; however, surgical intervention, particularly the use of large meshes and rigid fixation, often results in increased abdominal wall stiffness and reduced mobility.
Abdominal walls that have been repaired are often much stiffer than healthy or even herniated ones. Larger mesh sizes are associated with less movement of the rectus abdominis during activities such as breathing. This loss of mobility is not just evident on scans; patients also report increased stiffness and discomfort, which can make it harder for them to return to physically demanding jobs.
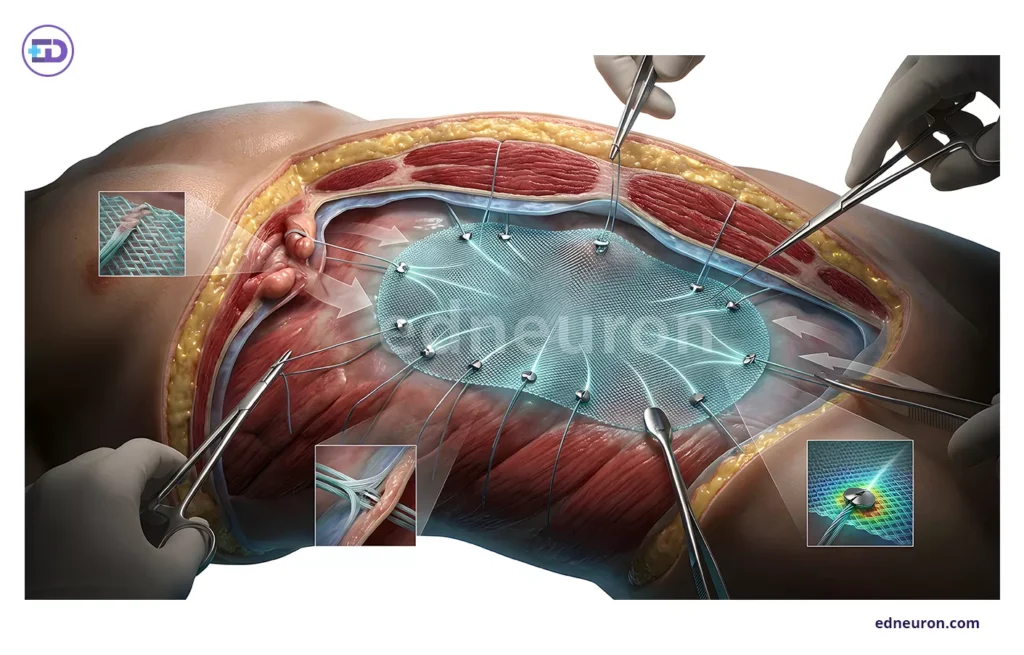
Fig 1: Suture fixation of a prosthetic mesh during an open ventral hernia repair.
Comparative Clinical Outcomes: Adhesion vs. Suturing
The clinical imperative to reduce penetrating trauma has led to the validation of tissue adhesives in the retromuscular space. A landmark retrospective review comparing TA (utilizing n-butyl-2 cyanoacrylate) and TS in major abdominal wall reconstruction (AWR) revealed that tissue adhesion is linked with significantly shorter operative times and a lower incidence of early postoperative complications. In the study, the mean operative time was reduced by approximately 40 minutes in the TA group compared to the suture group (101.8 vs. 141.2 minutes), reflecting the technical efficiency of non-mechanical fixation.
More importantly, patients in the suture group had much higher rates of severe postoperative pain (VAS 7-10) than those in the adhesive group (30.4% vs. 3.5%). This means that avoiding trans-fascial sutures may be the best way to prevent long-term, severe pain after hernia repair. Importantly, using adhesives does not seem to make the repair less durable. After 24 months, recurrence rates are similar for both methods, with some evidence even favoring adhesives (3.5% vs. 8.6%).
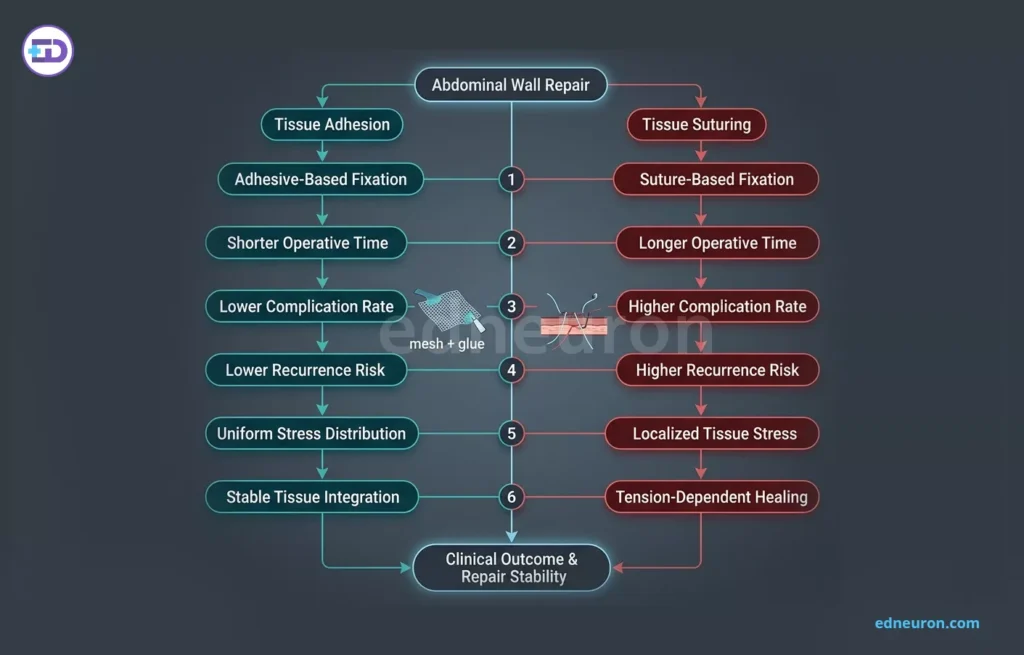
Fig 2: Comparative analysis of mesh fixation methods showing the clinical advantages of adhesive-based adhesion (cyan) over suture-based suturing (red) across key procedural outcomes.
Clinical Interpretation and Practical Implications
For the clinician, these findings suggest a paradigm shift. If microporous synthetic meshes integrate rapidly within a well-vascularized retromuscular space, the shear force provided by the integrated mesh may eventually offload the tension on the closed defect site, rendering aggressive trans-fascial fixation redundant. The primary role of fixation is therefore to prevent mesh migration in the immediate postoperative period rather than to provide long-term structural tension.
Reducing chronic pain has a big impact on patients’ lives and finances. Studies show that ongoing pain after complex hernia repair can cause people, especially manual workers, to lose their sense of job identity and face financial problems. By using less traumatic fixation methods, such as tissue adhesives, surgeons can help patients return to work sooner and improve their quality of life. This is now seen as an important measure of surgical success.
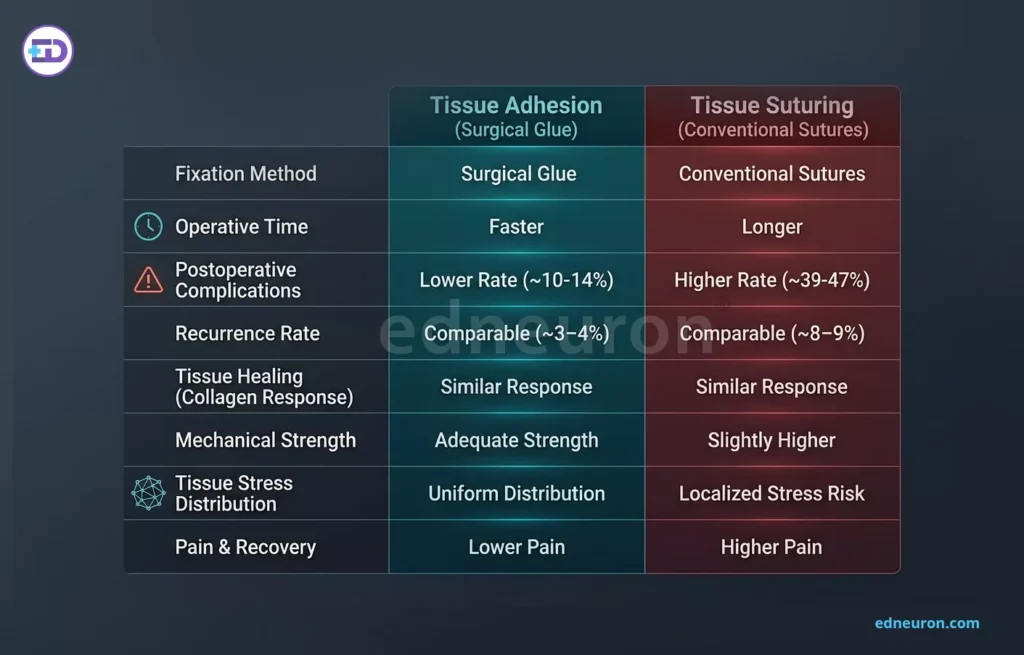
Fig 3: This table compares the clinical outcomes of tissue adhesion using surgical glue versus conventional tissue suturing in abdominal wall repair.
Limitations and Uncertainty
Despite these promising results, several gaps in the evidence remain. Most comparative studies on TA vs. TS involve small, retrospective cohorts, which may be subject to selection bias. Additionally, there is a lack of standardization in the measurement of “abdominal wall function” perioperatively. While muscle strength is frequently assessed, other domains such as trunk mobility and core stability are often overlooked, limiting our ability to fully characterize the functional impact of different fixation methods.
Conclusion
Switching from mechanical sutures to biological adhesives marks a step forward in abdominal wall reconstruction, focusing more on natural function than just strength. Current evidence shows that tissue adhesives are safe and effective, helping shorten surgery time and reduce severe postoperative pain without increasing the risk of a hernia recurrence. Clinicians should keep these benefits in mind, especially for working-age patients who need to recover quickly.
References
- Shaikh S, et al. A clinical study of anterior abdominal wall hernias and its management. Cureus. 2024;16(8):e11410062. Available from:
- Khan M, et al. A review of abdominal meshes for hernia repair—current status and emerging solutions. Materials (Basel). 2023;16(21):6798. doi:10.3390/ma16216798
- De Maria C, et al. Abdominal wall hernia repair: from prosthetic meshes to smart materials. Bioengineering (Basel). 2023;10(6):685. Available from:
- Singh A, et al. Abdominal wall hernias: an epidemiological profile and surgical experience from a rural medical college in central India. Surg J (N Y). 2021;7(2):e90–e95.
- Petro CC, et al. A scoping review of abdominal wall functional assessment in patients with hernias. Hernia. 2025. doi:10.1007/s10029-025-03517-2
- Köckerling F, et al. Novel insights into abdominal wall hernia and its negative impact on patients’ finances. Hernia. 2026. doi:10.1007/s10029-026-03596-9
- Biomechanics of the abdominal wall before and after ventral hernia repair using dynamic MRI. arXiv. 2026.
- Smith J, et al. Mesh fixation in abdominal wall reconstruction: a retrospective review. World J Surg Surg Res. 2024;7:1456.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



