

Introduction
The surgical management of acute appendicitis, a condition with a lifetime risk of approximately 7-8%, has undergone a paradigm shift over the last four decades. Since McBurney first described the muscle-splitting incision in 1894, open appendectomy (OA) served as the unchallenged gold standard, prized for its therapeutic efficacy and low mortality. However, the advent of laparoscopic appendectomy (LA) has introduced a profound clinical tension: does the preservation of the abdominal wall through minimally invasive access trade off the thoroughness of peritoneal debridement, particularly in complicated cases? What emerges from the evidence is not a simple victory of one technique over another, but a nuanced hierarchy of outcomes that depends heavily on the inflammatory stage of the disease and the patient’s specific demographic.
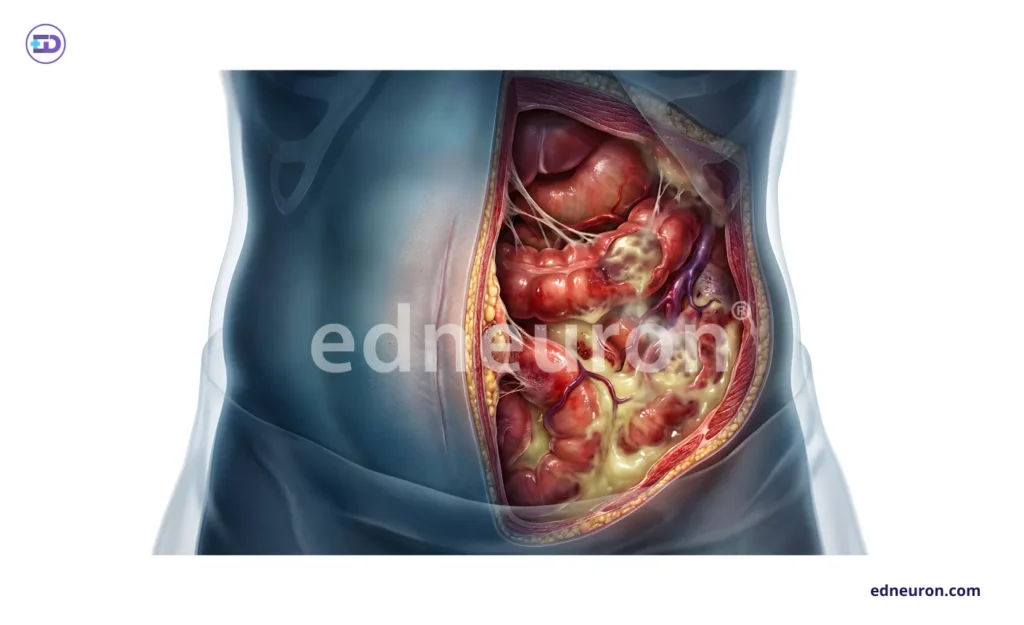
Fig 1: Anatomical pathology of acute appendicitis and peritonitis, highlighting the surgical challenge of optimizing recovery speed while mitigating deep-space infectious risks.
The Paradox of Wound Integrity vs. Intra-abdominal Sepsis
The primary analytical dilemma in current surgical practice concerns the discordant risk profiles of LA and OA for infectious complications. Meta-analytical data involving over 7,600 patients demonstrate that LA provides a robust protective effect against surgical site infections (SSIs), with a Peto odds ratio of 0.42. This is likely a mechanical consequence of retrieving the inflamed specimen through a trocar sleeve, thereby shielding the abdominal wall from direct contamination.
However, this superficial benefit has historically been shadowed by a persistent concern: a significantly increased incidence of intra-abdominal abscesses (IAAs) following the laparoscopic approach in adults. While IAAs are recognized by prolonged ileus and spiking fevers, the mechanism behind this increase remains debated—potential factors include the aerosolization of bacteria or inadequate dependent drainage during the pneumoperitoneum. Interestingly, this deep-space risk appears to be age-dependent; in pediatric populations, LA does not show a statistically significant increase in IAAs and may even trend toward a reduction in deep-space sepsis.
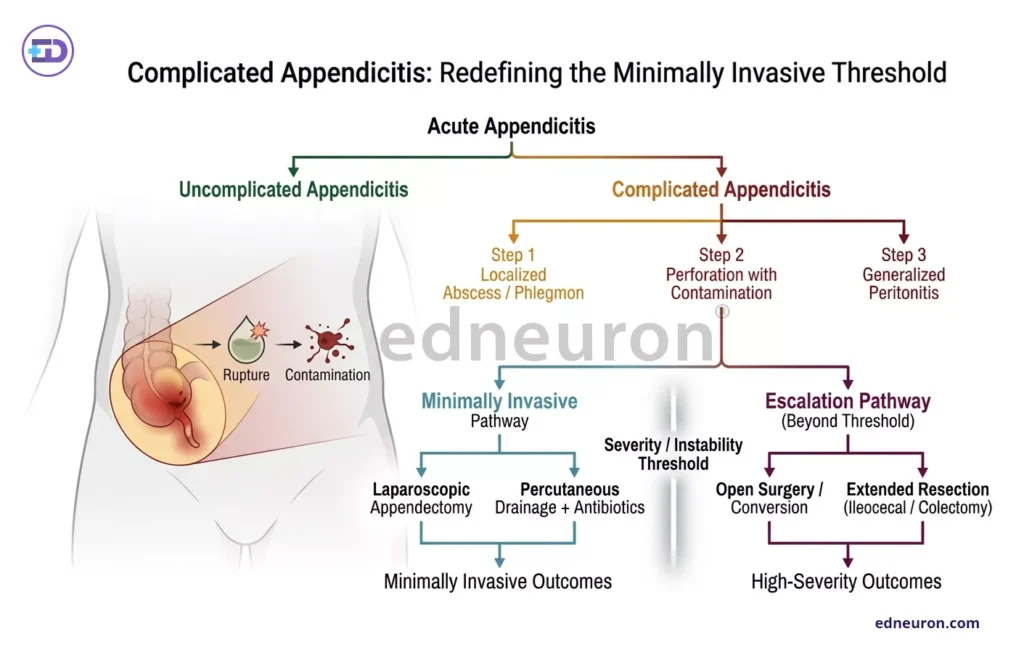
Fig 2: Flowchart detailing the treatment pathways and outcomes for different severity levels of acute appendicitis.
Complicated Appendicitis: Redefining the Minimally Invasive Threshold
The debate intensifies when addressing “complicated” appendicitis (CA), defined by perforation, gangrene, or abscess formation, which accounts for nearly 20% of presentations and carries higher morbidity. Historically, surgeons favored the open approach for CA to ensure tactile feedback and extensive irrigation. Yet recent single-center audits and meta-analyses suggest that the “minimally invasive advantage” may be more pronounced in high-risk scenarios.
Laparoscopy allows for superior visualization of the entire peritoneal cavity, facilitating the detection of unexpected pathology and more comprehensive peritoneal toileting. Clinical outcomes in CA patients treated laparoscopically include significantly lower rates of postoperative ileus—7.1% compared to 26.3% in open cases—and a shorter hospital stay. This suggests that the reduction in bowel manipulation and the attenuated inflammatory stress response associated with laparoscopy are critical drivers of gastrointestinal recovery.
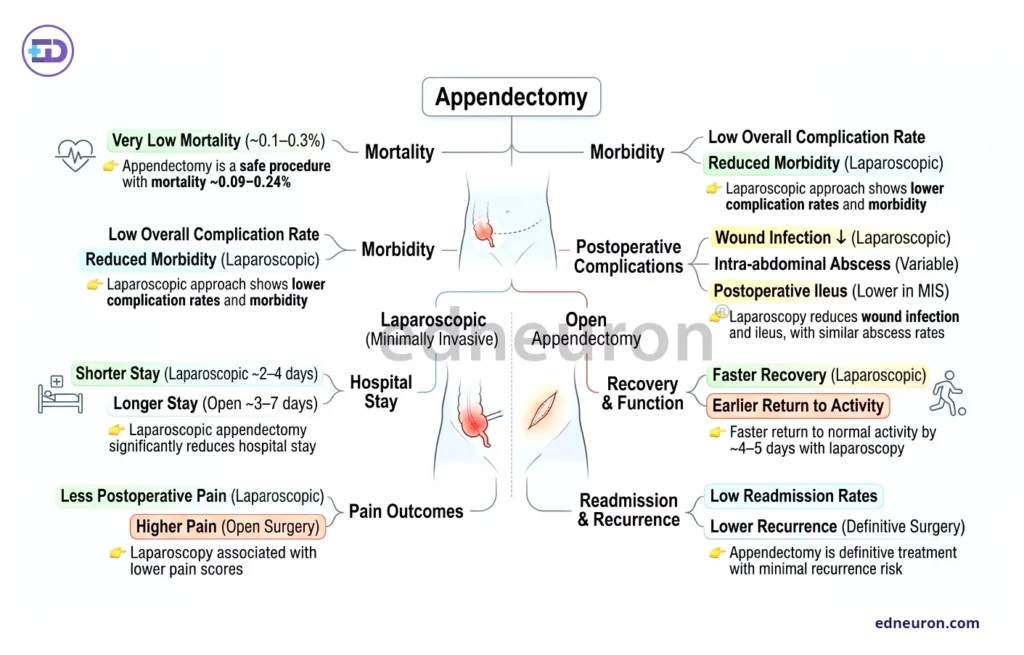
Fig 3: Overview of comparative clinical outcomes and recovery metrics for laparoscopic versus open appendectomy.
Clinical Outcomes and Real-World Implementation
The transition from mechanism to clinical reality reveals a clear victory for LA in terms of recovery velocity. Adults undergoing LA return to normal activity approximately five days earlier than those treated with OA. From a systems perspective, the median length of stay is reduced by approximately 1 day, an effect that is consistent across various healthcare environments.
The utility of LA is particularly evident in specific “blind spot” populations:
- Obese Patients: The technical ease of laparoscopy avoids the challenges of deep incisions in thick subcutaneous fat, resulting in faster recovery and fewer wound complications.
- Young Females: Given the high rate of diagnostic uncertainty and the potential for gynecological mimickers, the broader abdominal exploration provided by LA increases the rate of definitive diagnosis.
Conclusion
While the Cochrane data remains a cautious reminder of the potential for deep-space complications in adults, the broader clinical trajectory favors the laparoscopic approach. LA is no longer merely a “modern” alternative; it is a safe and effective methodology that redefines the recovery curve. However, the deep-space safety of LA is not an inherent property of the technology but a reflection of surgical expertise. As residency training expands, the silent variable in the intra-abdominal abscess equation—the learning curve—will likely dissipate, leaving laparoscopy as the undisputed standard for both simple and complex appendectomies.
References
- Patel, V., Mehta, N., & Shah, P. (2021). Retrospective analysis of laparoscopic versus open appendectomy for acute appendicitis. International Surgery Journal, 8(3), 912–916.
- Al-Mulhim, A. A., & Al-Mulhim, F. M. (2024). Surgical outcomes of emergency open appendectomy for acute appendicitis: A retrospective cohort study. Cureus, 16(2), e12003998.
- Singh, R., Verma, S., & Kulkarni, P. (2025). Comparison of laparoscopic and open appendectomy outcomes in acute appendicitis. Journal of Trends in Medical Investigation, 2(1), 1–7.
- Ahmed, I., Khan, M., & Rehman, A. (2024). Laparoscopic versus open appendectomy in complicated and uncomplicated appendicitis: A comparative study. Cureus, 16(3), e12433581.
- Sauerland, S., Jaschinski, T., & Neugebauer, E. A. (2010). Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database of Systematic Reviews, (10), CD001546.
- Sauerland, S., Lefering, R., & Neugebauer, E. A. (1998). Laparoscopic versus conventional appendectomy: A meta-analysis of randomized controlled trials. Langenbeck’s Archives of Surgery, 383(3–4), 289–295.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



