

Introduction
Infective endocarditis (IE) has a prevalence of about 10-20% in modern times, and the clinician’s ability to act decisively hinges on microbiologic certainty to institute treatment; however, such definitive cultures are not always available. 5% to 30% of suspected IE cases are persistently negative, creating a void with direct and serious implications for timely microbial management, surgical scheduling, and prognosis. Blood culture–negative endocarditis (BCNE) is a heterogeneous amalgamation characterized by cultures that fail to yield a pathogen. Managing it demands not only thorough knowledge of fastidious organisms and alternative diagnostic platforms, but also the intellectuality to operate under uncertainty without prematurely closing the diagnostic loop.
Pathophysiology And Etiologic Spectrum
The 3 common precipitants of this blood culture-negative endocarditis are
- Use of antimicrobials before sample collection for blood culture
- The HACEK group of organisms and nutritionally variant streptococci (Granulicatella spp., Abiotrophia defectiva) fail to grow under standard laboratory conditions.
- The true BCNE: due to intracellular organisms replicating within the macrophages that cannot be cultured using traditional techniques (Coxiella burnetii, the agent of Q fever endocarditis). In such cases serologic detection of phase I IgG antibodies above a titer of 1:800 remains the diagnostic cornerstone.
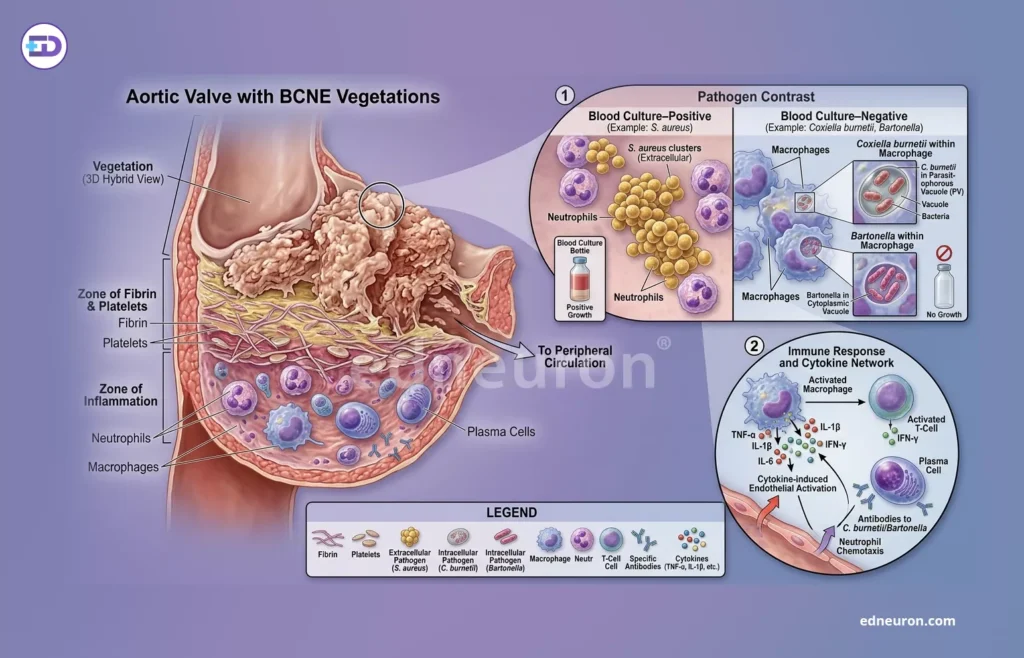
Fig 1: In the case of BCNE, the pathogen is intracellular in aortic valve vegetations and thus not culturable.
The most common in contemporary practice is prior antibiotic exposure, a modifiable yet frequently encountered confound that suppresses bacteremia without eradicating valvular infection. The 2023 Duke–International Society for Cardiovascular Infectious Diseases (ISCVID) criteria added PCR, amplicon, and metagenomic sequencing for organisms that are least susceptible to culture, such as Bartonella species. Tropheryma whipplei, the cause of Whipple disease, should be considered in cases with systemic features disproportionate to valvular pathology, and confirmed by 16S rRNA sequencing or specific PCR. Fungal endocarditis, HACEK organisms, and non-bacterial thromboembolic endocarditis, including Libman-Sacks endocarditis in antiphospholipid syndrome and marantic endocarditis in malignancy, complete a differential that demands systematic rather than reflexive evaluation.
Diagnostic Challenges
The original Duke criteria and their 2000 modification were constructed around blood culture positivity as a major criterion, thereby rendering them structurally disadvantaged in BCNE. A case series by Lamas CC et al. 2003 demonstrated that, for pathologically proven cases, the Duke criteria correctly identified only 21% of native disease and 45% of the prosthetic valve variant. The 2023 Duke-ISCVID criteria represent a substantive revision:
- Incorporation of PCR and amplicon or metagenomic sequencing results from blood or valve tissue for a fastidious organism.
- Coxiella and Bartonella serology as independent major criteria
- Fluorodeoxyglucose positron emission tomography with computed tomography (FDG-PET/CT) and cardiac CT as imaging major criteria
- Extending the framework to prosthetic valve and cardiac device infection.
The revised criteria do not eliminate diagnostic ambiguity; they formalize a more honest accounting of the evidence available—and in doing so, expose how much of BCNE diagnosis has historically rested on clinical gestalt rather than validated criteria.”
For prosthetic valve disease and cardiac device infection, advanced imaging modalities- FDG-PET/CT have proven most informative due to their high sensitivity and specificity. In contrast, echocardiography is the least reliable and is used to map extracardiac embolic foci that confirm systemic septic seeding. It must be duly noted that a negative PET/CT scan cannot exclude native valve endocarditis, particularly in early or treated disease, and clinicians who over-rely on imaging to rule out IE in culture-negative cases risk the exact diagnostic error they sought to avoid.
Clinical Implications
The tension at the center of BCNE management is not merely diagnostic—it is therapeutic.
The archetypal culture-positive phenotype, treated with first-line empirical antimicrobials, does not work against intracellular organisms such as Coxiella burnetii (Q fever endocarditis), which requires prolonged doxycycline-hydroxychloroquine combination therapy, often for 18 months or more in native valve disease. Starting an empirical regimen without an etiologic diagnosis is almost like shooting in the dark, which delays operative intervention in patients with clear surgical indications. So optimizing blood culture yield, pursuing serology and molecular diagnostics in parallel, and escalating to tissue-based methods when surgery is performed form the cornerstone of effective BCNE management. This framework underscores the efficiency and importance of a dedicated multidisciplinary endocarditis team and forms the structural standard for complex IE, including BCNE.
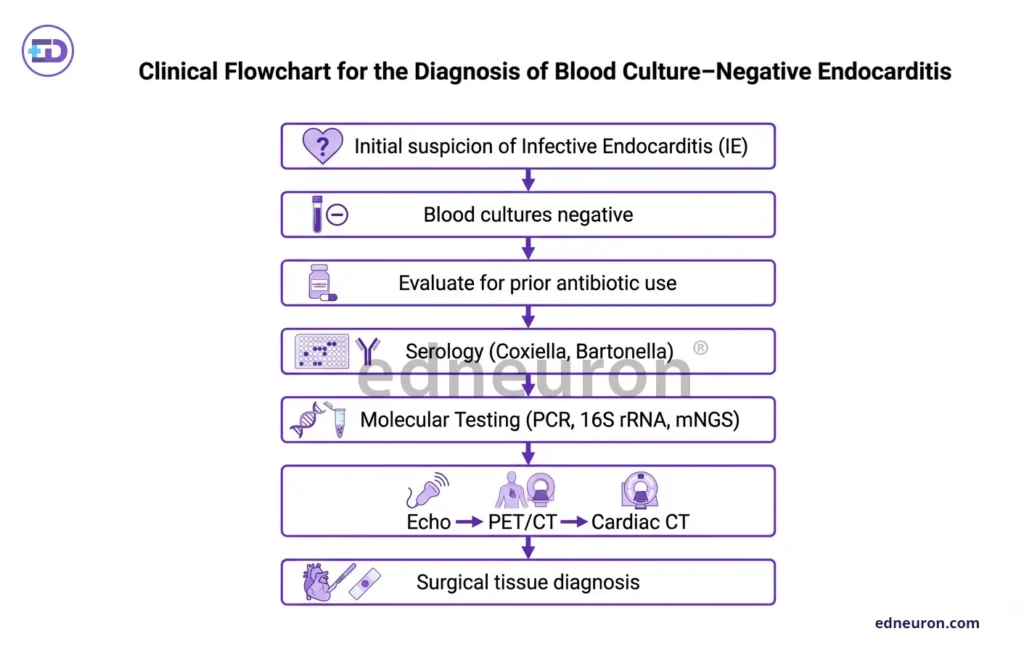
Fig 2: Evaluation strategy.
Conclusion
Blood culture-negative endocarditis occupies the critical intersection of microbiologic uncertainty, diagnostic technology, and high-stakes decision-making.
The revision in diagnosis is witnessing a paradigm shift from a culture-specific to multimodal inclusion of advanced nuclear medicine imaging, tissue characterization, and serology. In BCNE, acknowledging uncertainty is not a failure of reasoning and is sometimes also inevitable. The appropriate take is one of structure: applying the diagnostic algorithm systematically, documenting the limits of available evidence, and resisting the reflex to force diagnostic closure.
References
- McHugh J, Saleh OA. Updates in Culture-Negative Endocarditis. Pathogens. 2023 Aug PMID: 37623987.
- Fowler VG, Durack DT, Selton-Suty C et al. The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria. Clin Infect Dis. 2023 Aug PMID: 37138445.
- Lamas CC, Eykyn SJ. Blood culture negative endocarditis: analysis of 63 cases presenting over 25 years. Heart. 2003 Mar;. PMID: 12591823.
- Ten Hove D, Slart RHJA, Sinha B et al. 18F-FDG PET/CT in Infective Endocarditis: Indications and Approaches for Standardization. Curr Cardiol Rep. 2021 Aug; PMID: 34363148.
- Kersh GJ. Antimicrobial therapies for Q fever. Expert Rev Anti Infect Ther. 2013 Nov. PMID: 24073941.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



