

HFpEF: a Diagnostic Landfill
Heart failure with preserved ejection fraction (EF equal to or more than 50%), accounting for more than half of heart failure cases, is considered the least specific diagnostic category, inclusive of a heterogeneous patient population- from metabolic hypertensive remodeling to hypertrophic cardiomyopathy, restrictive physiology, and infiltrative disease. A meta-analysis of 5 studies involving more than 600 patients (Magdi M et al., 2022) identified ATTR-CM (transthyretin amyloidosis) in approximately 11% of patients previously categorized as HFpEF. This, when applied to the epidemiologic scale of HFpEF in the United States, represents hundreds of thousands of patients misclassified as having a hemodynamic syndrome when they have a progressive molecular disease. Prospective screening using DPD scintigraphy identified wild-type ATTR-CM in 8% of undifferentiated HFpEF patients who had not previously been referred for amyloid evaluation. Most of these were older males with increased LV thickness and elevated high-sensitive troponin levels. ATTR-CM is a proteostatic disease in which unstable or misfolded oligomers of transthyretin or C-terminal proteolytic activities destabilize their native tetrameric configuration, aggregate into amyloid fibrils/protofilaments/other intermediates, and infiltrate the myocardial extracellular matrix as mechanically inert, electrically hostile, and progressively space-occupying deposits. Amyloid infiltration, especially with a predilection for the basement membrane (abundant in collagen IV, laminin, and fibronectin), impairs diastolic filling, induces atrophy and degeneration of myocardial cells, inducing cardiac conduction abnormalities while preserving systolic shortening fraction until late disease, generating the exact hemodynamic signature that HFpEF criteria were designed to identify. The signature capture is almost too perfect, and that perfection is precisely the problem: HFpEF absorbs ATTR-CM without triggering the molecular investigation the disease requires.
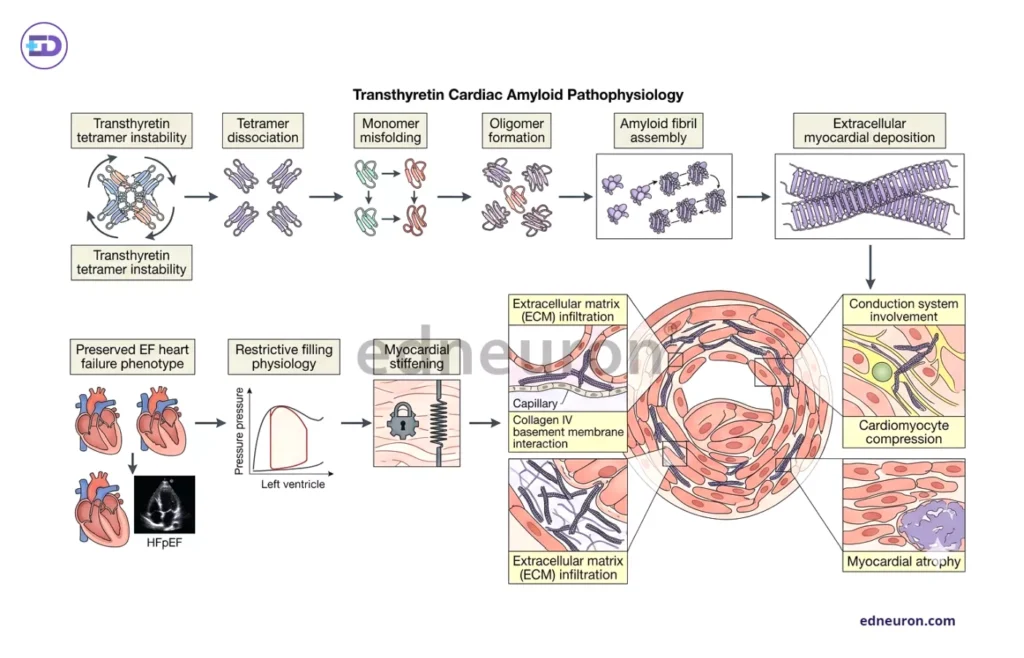
Fig 1 : Pathophysiology of ATTR-CM.
Consider this case in IPD
A man who is 70 years old, hypertensive, with a history of bilateral carpal tunnel releases and a laminectomy for lumbar stenosis, presents with progressive exertional dyspnea and peripheral edema.
Echocardiography: concentric left ventricular thickening with an EF of 58%. ECG: low QRS voltage along with a pseudoinfarction pattern.
The differential that is considered is hypertensive heart disease and heart failure with preserved ejection fraction, so the patient is started on a diuretic and discharged with instructions to follow a low-sodium diet. The diagnosis is unlikely to be correct as this patient has the cardinal syndromic features of wild-type transthyretin amyloid cardiomyopathy: orthopedic soft-tissue amyloid deposits preceding cardiac involvement, voltage-mass discordance on electrocardiography, and a pattern of wall thickening inconsistent with the hemodynamic history. The disease announced itself orthopedically and electrophysiologically years before it declared itself cardiologically.
RED-FLAG CONSTELLATION FOR ATTR-CM WITHIN HFpEF
The following multisystem features should trigger active ATTR-CM evaluation in any older patient with HFpEF or unexplained LV wall thickening:
Cardiac features:
- Unexplained LV hypertrophy
- Low-flow low-gradient aortic stenosis
- Preserved Ejection Fraction with restrictive filling (blunted x descent)
- Higher levels of NT-pro BNP (N-terminal pro B-natriuretic peptide)
ECG:
- Low QRS voltage despite increased wall thickness (voltage-mass discordance)
- Pseudo-infarction pattern
Extracardiac features:
- Analysis of tenosynovial tissues reveals bilateral carpal tunnel syndrome.
- Spinal canal stenosis, suggesting amyloid deposition in ligaments
- Peripheral or autonomic neuropathy
- Bilateral lower extremity edema
- Spontaneous biceps tendon rupture
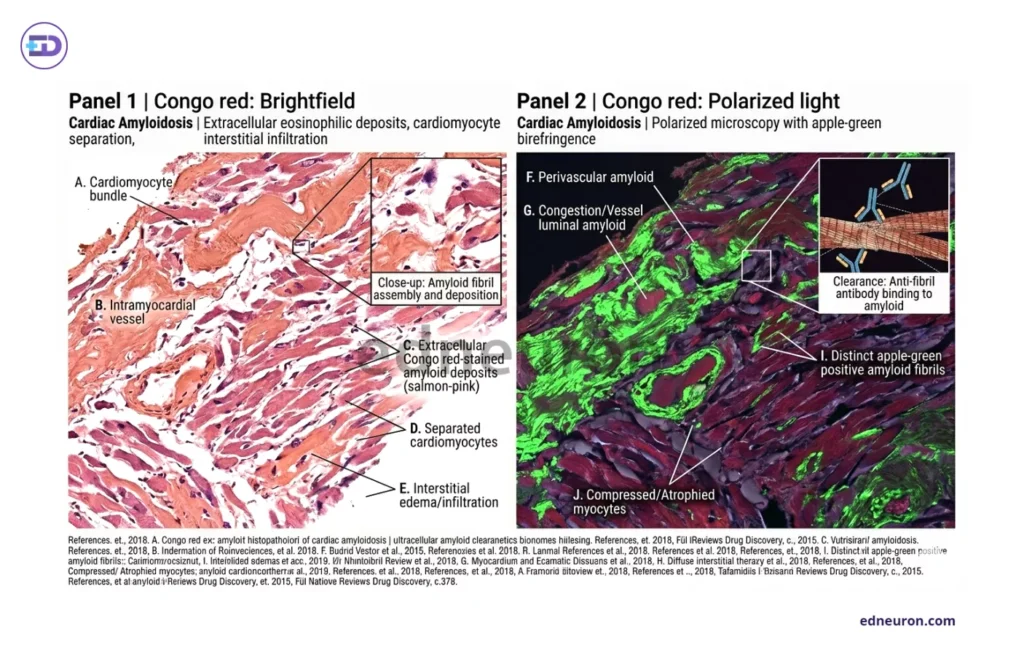
Fig 2 : Pathological slide of cardiac amyloidosis.
The Multisystem Red-Flag Signature and Its Clinical Neglect
ATTR-CM begins in connective tissues and peripheral nerves, where misfolded transthyretin aggregates in their extracellular compartments are deposited. Bilateral carpal tunnel syndrome, on tenosynovial analysis, reveals amyloid aggregation preceding cardiac diagnosis in a substantial proportion of wild-type ATTR-CM patients, sometimes by a decade or more. Wild-type Amyloid infiltration of the ligamentum flavum has been identified in pathologic specimens from 13% of patients undergoing decompressive laminectomy for spinal stenosis (SS), and was found with occult ATTR-CM documented in a subset. This transforms a routine orthopedic procedure into a potential encounter for a biomarker. Peripheral/autonomic neuropathy, spontaneous biceps tendon rupture, and refractory bilateral edema, along with GI and renal problems, constitute a constellation of disconnected clinical findings that gallop across orthopedics, neurology, musculoskeletal, and cardiology; the patient ends up seeing 5 physicians before an accurate diagnosis is made. ATTR-CM misdiagnosis rates have been documented at levels exceeding 39% in contemporary surveys, with patients receiving treatment for incorrect diagnoses (hypertension, hypertrophic cardiomyopathy, idiopathic restrictive cardiomyopathy for the putative LV thickening or even Aortic stenosis left ventricular hypertrophy) before a correct molecular diagnosis is established. The survey found that fewer than 10% of practitioners systematically screen HFpEF patients for cardiac amyloidosis (AL and ATTR), despite many reporting prior experience diagnosing the disease. This shows exactly what the structural problem is-the knowledge is present, but the clinical reflex to apply it systematically has not been built.
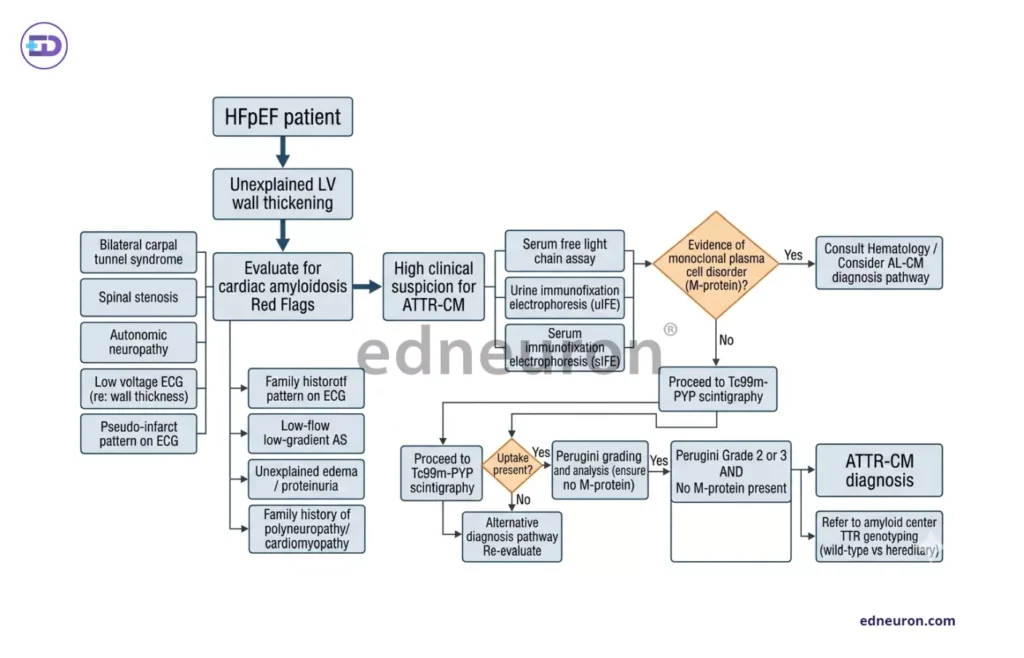
Fig 3 : Workflow of evaluating and diagnosing a patient suspicious of ATTR-CM
Voltage-Mass Discordance and the Electrophysiologic Announcement
Low QRS voltage coexisting with echocardiographic left ventricular wall thickening in 25-40% of patients with ATTR-CM and in 68% of patients with AL-CM; this electrocardiologic paradox deserves particular mention. Myocardial hypertrophy increases the girth of the ventricular wall and, correspondingly, electrical vector summation. In cardiac amyloidosis due to amyloid infiltration, unstable amyloid oligomers physically displace cardiomyocytes, induce atrophy, and insulate the heart with inert fibrillar deposits. However, in ATTR, where the amyloid burden is higher than in AL, and AL still shows higher characterization with LQRS, this suggests that QRS attenuation occurs in response to inflammation, edema, pericardial effusion, and other mechanisms beyond amyloid insulation.
From Biopsy to Bone Scintigraphy
The technical barriers to ATTR-CM diagnosis have been substantially dismantled as evidenced by the seminal 2016 analysis by Gillmore JD et al. established that Tc-99m pyrophosphate and Tc-99m scintigraphy, combined with exclusion of monoclonal protein by serum free light chains and serum and urine immunofixation electrophoresis, achieves a 100% positive predictive value for ATTR-CM with grade 2 or 3 uptake (Perugini Score) with sensitivity >99% and specificity of 86%. Thus forming the cornerstone of noninvasive diagnosis for the majority of patients. Advanced echocardiographic strain imaging has added a complementary functional layer. Deformation patterns: the apical-sparing pattern on longitudinal strain analysis, global longitudinal/radial/circumferential strain has been incorporated into current multimodality diagnostic algorithms as a triage tool to better differentiate CA from hypertrophic hearts, though it has limited sensitivity and cannot be used as a rule-out test. Cardiac magnetic resonance imaging CMR and extracellular volume mapping provide additional characterization of amyloid burden with lower interobserver variability except for cases of arrhythmias and cardiac devices acting as artifacts; the prognostic value remains beyond the diagnostic binary. The 2023 American College of Cardiology Expert Consensus Decision Pathway developed a multimodality algorithm for the identification of red-flag constellation, nuclear medicine scintigraphy, and tissue typing. The missing ingredient, more often than not, for prompt diagnosis is clinical suspicion
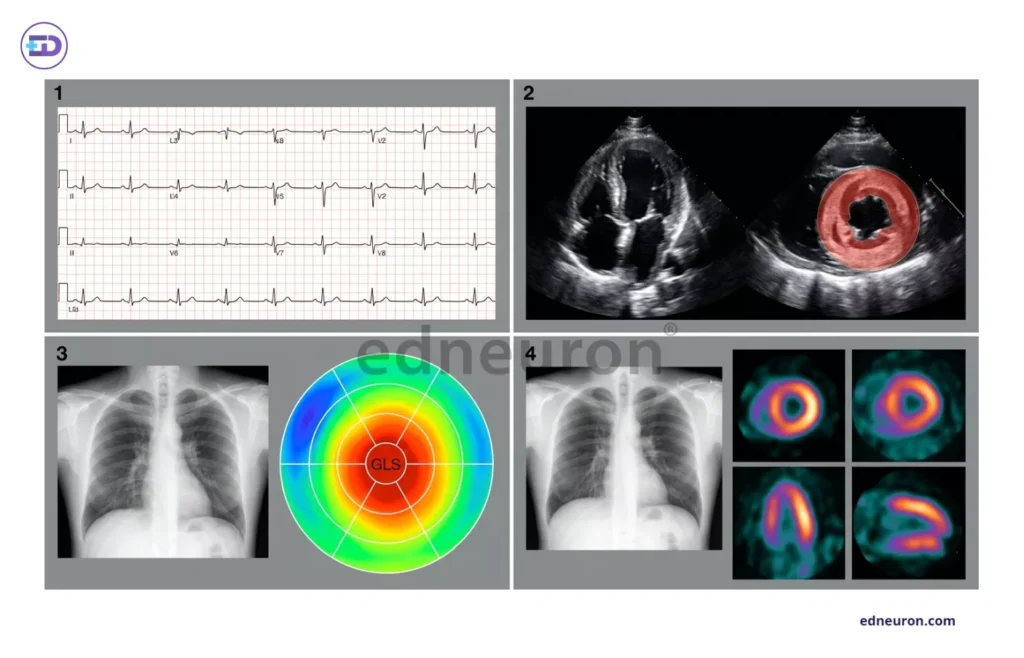
Fig 4 : 1) Low QRS voltage despite increased myocardial wall thickness (voltage–mass discordance), a characteristic electrophysiologic clue in cardiac amyloidosis. 2) Echocardiography demonstrating increased left ventricular wall thickness with concentric restrictive remodeling. 3) Chest radiography with accompanying global longitudinal strain (GLS) bull’s-eye strain map demonstrating the classic “apical sparing” pattern (“cherry-on-top” appearance). 4) Bone scintigraphy demonstrating increased myocardial radiotracer uptake,.
Therapeutic Urgency and the Ethical Weight of Missed Diagnosis
The ethical and clinical stakes of the diagnostic gap have been transformed by the emergence of effective disease-modifying therapy. Tafamidis, a small-molecule transthyretin tetramer stabilizer, demonstrated in the ATTR-ACT trial a 30% relative reduction in all-cause mortality and significant reductions in cardiovascular hospitalizations over 30 months of follow-up, being the first pharmacologic agent to alter the history of ATTR-CM. Vutrisiran is a small interfering RNA (siRNA) agent that impedes hepatic transthyretin synthesis, interefering-degrading-lowering TTR levels, highlighting experimentation with disease-modifying agents in the sphere that approaches disease modification via decreased production rather than conformational stability. An expanding pipeline, including acoramidis, patisiran, and investigational anti-fibril monoclonal antibodies, underscores the depth of translational investment now directed at the full mechanistic spectrum of ATTR-CM. When ATTR-CM was a disease without effective treatment, diagnostic delay represented a failure of prognosis but not of therapeutic opportunity.
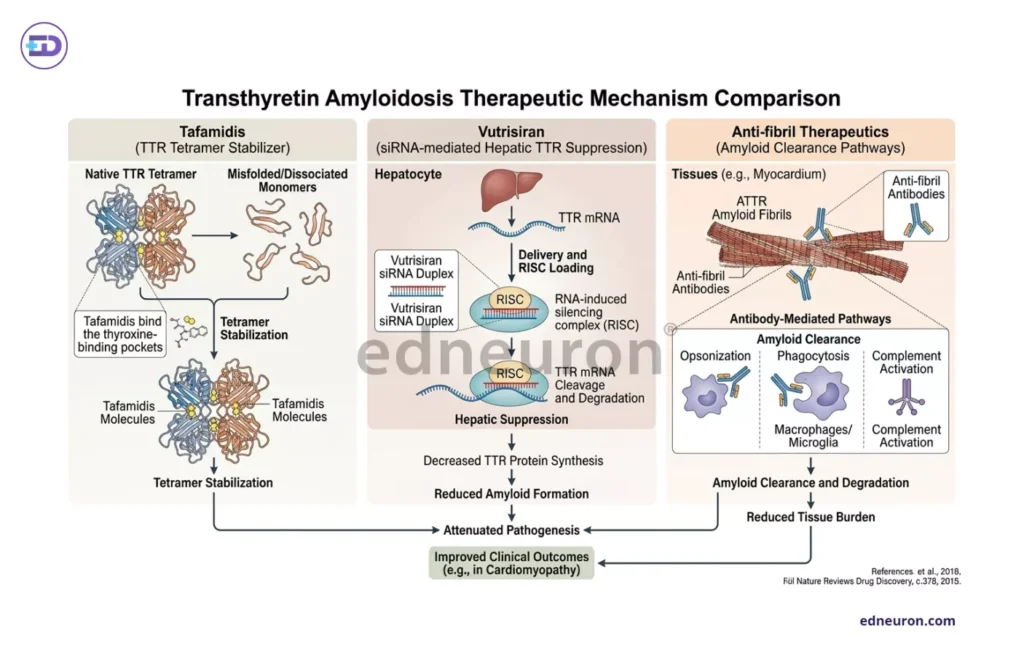
Fig 4 : Various therapeutic modalities for improved clinical outcomes.
The Diagnostic Gap We Can No Longer Ignore
In the current era of modern pharmaceuticals, delayed diagnosis denies patients access to agents that demonstrably extend survival and reduce the burden of heart failure hospitalization. The patient, categorized under HFpEF and treated with diuretics alone, in whom ATTR-CM slipped slimy out of suspicion, despite bilateral carpal tunnel surgery and lumbar decompression, is a patient with a smoke-wisp memory of hope, with a potential window for extended survival, not worked upon.
The armamentarium with its red-flag signs, non-biopsy diagnostic procedures, and the disease-modifying agents that cleared regulatory approval and demonstrated survival benefit in randomized trials. What must be inspired within the cardiologist’s consciousness is the reflex on encountering an older patient with unexplained wall thickening, bilateral orthopedic soft-tissue disease, and low electrocardiographic voltage, to think not ‘hypertensive heart disease with preserved ejection fraction’ but rather ‘this pattern requires molecular exclusion of transthyretin amyloidosis before a hemodynamic diagnosis is accepted. Building that reflex, through training/guideline implementation, and integration of ATTR-CM screening into HFpEF clinical pathways, is the imperative of the present moment in cardiovascular medicine.
References
- Magdi M, Mostafa MR, Abusnina W, et al. A systematic review and meta-analysis of the prevalence of transthyretin amyloidosis in heart failure with preserved ejection fraction. Am J Cardiovasc Dis. 2022 Jun 15;12(3):102-111. PMID: 35873185.
- Healy L, Giblin G, Gray A, et al. Prevalence of transthyretin cardiac amyloidosis in undifferentiated heart failure with preserved ejection fraction. ESC Heart Fail. 2025 Apr;12(2):1176-1182. PMID: 39508367.
- Godara A, Riesenburger RI, Zhang DX, et al. Association between spinal stenosis and wild-type ATTR amyloidosis. Amyloid. 2021 Dec;28(4):226-233. PMID: 34263670.
- Writing Committee; Kittleson MM, Ruberg FL, Ambardekar AV et al. 2023 ACC Expert Consensus Decision Pathway on Comprehensive Multidisciplinary Care for the Patient With Cardiac Amyloidosis: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2023 Mar 21;81(11):1076-1126. doi: 10.1016/j.jacc.2022.11.022. Epub 2023 Jan 23. Erratum in: J Am Coll Cardiol. 2023 Mar 21;81(11):1135. doi: 10.1016/j.jacc.2023.02.013. PMID: 36697326.
- Gillmore JD, Maurer MS, Falk RH, et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation. 2016 Jun 14;133(24):2404-12. PMID: 27143678.
- Maurer MS, Schwartz JH, Gundapaneni B, et al. ATTR-ACT Study Investigators. Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy. N Engl J Med. 2018 Sep 13;379(11):1007-1016. PMID: 30145929.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



