

From 2015-2025: What Changed?
The 2015 European Society of Cardiology Guidelines defined acute pericarditis by a deceptively simple formula: any two of four classic features.
- Pleuritic chest pain
- Pericardial friction rub
- Diffuse ST-segment elevation with PR-segment depression
- New or worsening pericardial effusion
When we trace the epistemic thought behind constructing such a framework, it naturally leads the design to prioritize sensitivity in an emergency setting, to avoid missing a crucial diagnosis, such as tamponade or partially treated myopericarditis. The problem that arose within such a system: a substantial proportion of patients diagnosed under these criteria lacked objective evidence of inflammation or a disease course consistent with inflammatory pericarditis, leading to unnecessary anti-inflammatory exposure and diagnostic inertia.
The 2025 ACC Expert Consensus Statement was restructured to rectify such fallacies, pleuritic chest pain that must be accompanied by at least more than one objective supportive feature drawn from a menu that explicitly incorporates inflammatory biomarkers.
- (C-reactive protein, erythrocyte sedimentation rate, cardiac troponin)
- Pericardial rub
- Multimodality imaging showing worsening or new pericardial inflammation or effusion (cardiac MRI, CT, echocardiography),
- Characteristic ECG changes (diffuse ST elevation and PR depression).
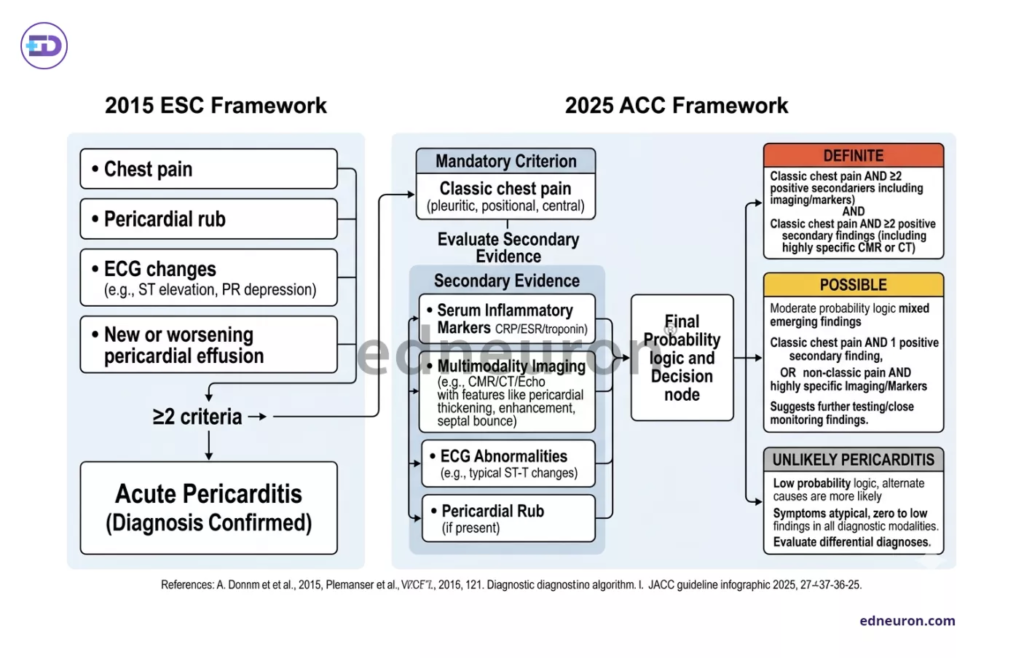
Fig 1 : Comparative panel of diagnostic framework 2015 ESC vs 2025 ACC.
The stepwise diagnostic scoring branches out to three probabilities: either definite, possible, or unlikely pericarditis, operationalizing what is, in essence, an adjudicating inflammatory framework. This shift from static categorization toward a probability-weighted, evidence-integrated construct, which parallels acute coronary syndrome and heart failure diagnostics, where syndromic presentations are anchored to biomarker and imaging evidence. The implications are:
- Such an approach improves diagnostic specificity
- There is attenuation of overdiagnosis
- Clinicians are now required to exercise longitudinal interpretive judgment rather than applying binary decision rules.
It is a test of time: whether this added complex multimodal approach can evolve into consistent diagnostic performance across heterogeneous clinical environments, emergency departments, and district cardiology outpatient services.
Cardiac MRI and the Invisible Inflammation
TTE, CCT, and Cardiac magnetic resonance imaging have become the investigative cornerstones for the diagnosis of pericarditis. Their integration into the routine algorithm represents both an advance and a new source of interpretive complexity in understanding and quantifying pericardial thickness (normal<2mm) and tamponade physiology. Some recognizable patterns of pericardial pathology are: T2 STIR-weighted edema on short-T1 inversion recovery sequences, white enhancement signal of effusion and septal bounce on cine white imaging with steady-state precision, and pericardial thickening. These modalities help track, diagnose, and prognosticate subclinical recurrence/occult inflammation in patients whose symptoms have seemingly resolved, with CRP below or at baseline. Such an earlier identification helps guide decisions around physical activity restriction and therapy tapering. The central dilemma, however, is whether MRI-visible inflammation in patients who are entirely asymptomatic and whose inflammatory markers have returned to baseline points towards the actual course of disease, a phenomenon that creates genuine imaging–symptom discordance. If the enhancement is treated as evidence of ongoing active inflammation, correlating with the patient’s clinical findings, it makes sense to continue or escalate anti-inflammatory therapy. If it is treated as a post-inflammatory residue without pathophysiological significance, it may be permissible to de-escalate, but that judgment lacks a validated evidence base. The newest evaluation strategy endorses decision-making without fully resolving this ambiguity, leaving clinicians as captains of their own teams to navigate on a case-by-case basis, using signal-dependent inference. Such rhetoric, which relies heavily on imaging studies, may lead to treatment decisions anchored to pixels rather than to physiology. The field of cardiology urgently requires prospective data that correlates MRI inflammatory parameters with recurrence and disease progression, and that data, as of 2025, remains completely limited by the lack of evidence and MRI-inflammatory threshold parameters.
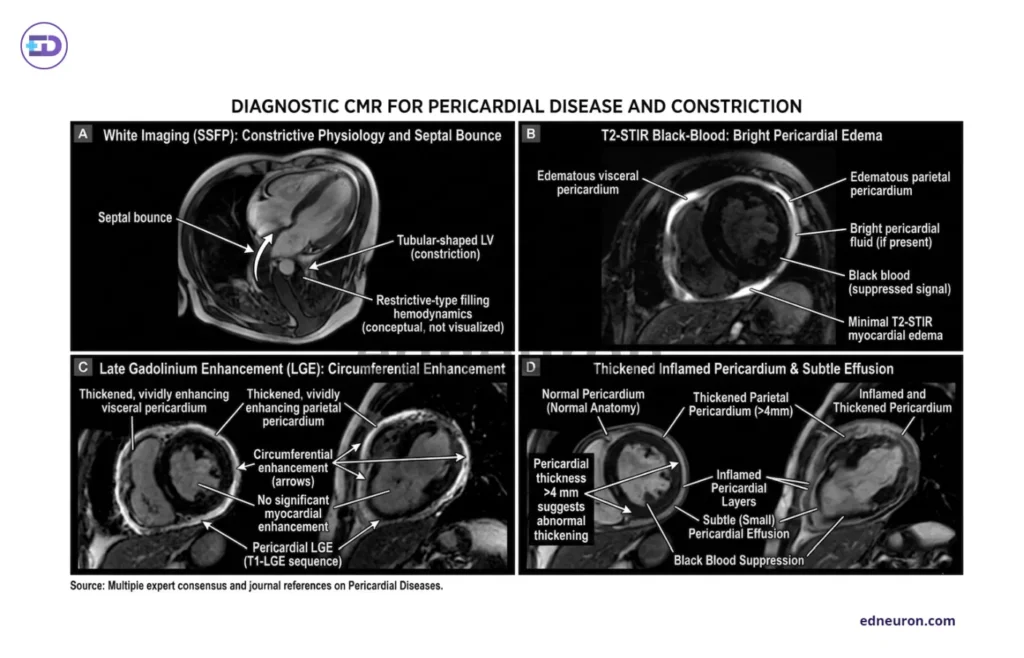
Fig 1 : A) Cine White Imaging (SSFP): Constrictive physiology and septal bounce. B) T2-STIR black-blood imaging showing hyperintense pericardial effusion. C) Late Gadolinium Enhancement (LGE) showing circumferential pericardial enhancement, inflamed visceral/parietal pericardium, viable dark myocardium. D) CMR: Increased pericardial thickness (>4 mm) supports constrictive pathology in the appropriate clinical context, although normal thickness does not exclude physiologically significant constriction.
Recurrent Pericarditis and the Emergence of an Autoinflammatory Phenotype
Recurrent pericarditis- defined as symptomatic relapse after a documented symptom-free interval of at least 4-6 weeks, and the frequency rises substantially with each subsequent recurrence. Approximately 15-30% of patients fall prey following the first episode. Possible etiologies include post-viral infectious syndrome, autoimmune flare, inadvertent corticosteroid-mediated perpetuation, and sensitization, which carries a hefty subset of patients under the conditions that develop out of dysregulated innate immunity signaling rather than adaptive immunity. The central focus of this model is the Interleukin-1 pathways, wherein the overexpression, transcription, and translation of the NLRP3 inflammasome lead to dysregulated constitutive activation of IL-1β, resulting in persistent inflammatory signaling in the pericardium and explaining both the recurrence pattern and steroid dependence of the refractory disease. We had two major trials documenting the implication of newer drugs for disease progression- the AIRTRIP trial established the triumph of IL-1 blockade: anakinra, a recombinant IL-1 receptor antagonist, reduced recurrences by approximately 94% compared with placebo in patients with colchicine-resistant, corticosteroid-dependent recurrent pericarditis. These patients were successfully tapered off from corticosteroid treatment, with CRP normalizing at day 8 and remaining so on day 60. The RHAPSODY trial also documented that rilonacept, a dimeric fusion protein that simultaneously traps IL-1α and IL-1β, reduced the annualized recurrence rate from 0.88 to 0.18 episodes per year (refer to Fig 3 below).
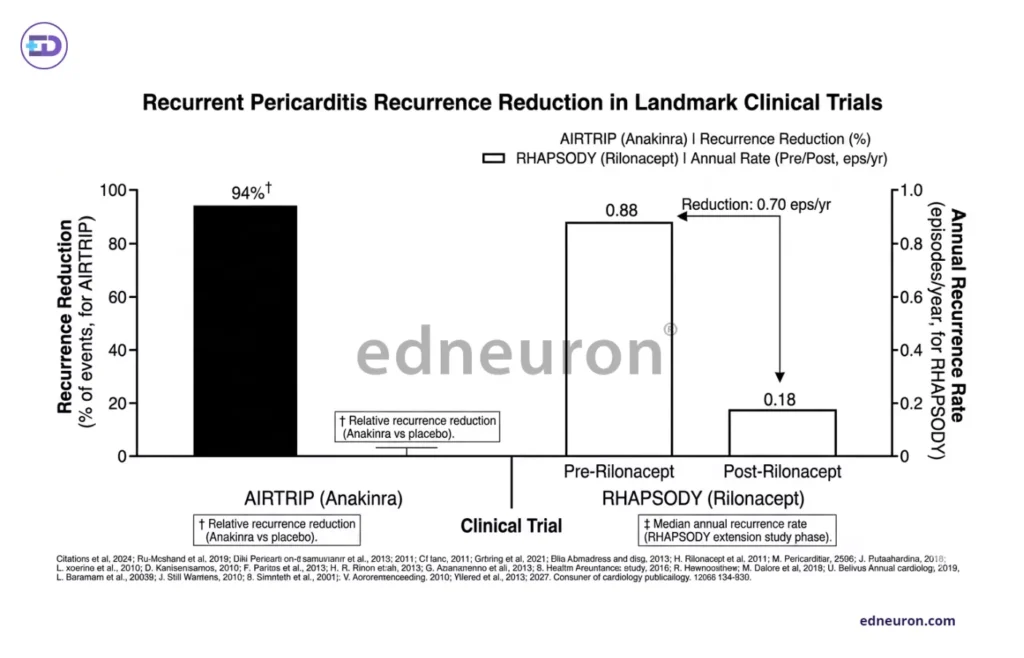
Fig 2 : Statistical representation of data in landmark clinical trials.
Such incredible results lead one to question whether these drugs are causing supression with exceptional potency of the residual autoinflammatory substrate, or whether they are truly modifying the course of the disease. Long-term study of rilonacept suggests that recurrence risk rises substantially after drug discontinuation in a significant proportion of patients, putatively implying the need to deliberate about the concept of operational remission, treatment duration, and cost effectiveness, a state in which patients remain clinically stable on maintained therapy without confirmed immunological quiescence.
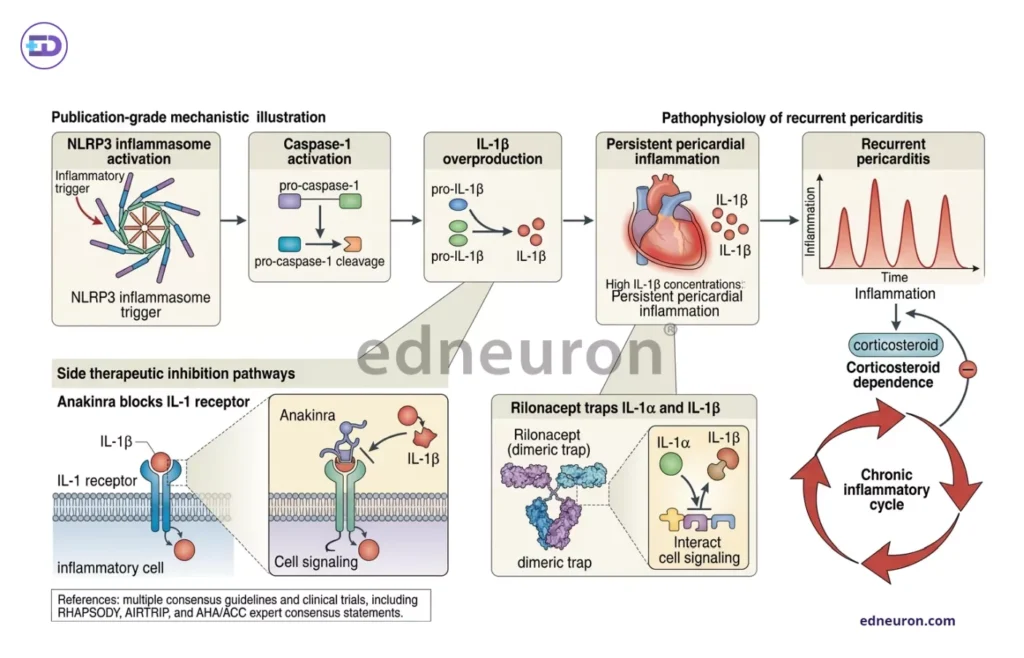
Fig 4 : Pathophysiology of Recurrent pericarditis and the newer drug modalities targeting specific steps in the inflammatory cascade.
Constrictive Pericarditis Vs Restrictive Cardiomyopathy
The differential diagnoses of constrictive pericarditis and restrictive cardiomyopathy constitute one of the most physiologically demanding exercises in clinical cardiology. Both these conditions present with similar clinical fingerprints/signs of bi-ventricular diastolic dysfunction, elevated filling pressures, and progressive systemic venous congestion, almost spitting mirror images, as one might say. When we wade through the physiology, we come across intriguing philosophies at work: the vena cavals are not affected by the swings of the intrathoracic pressure; constrictive pericarditis, characterized by ventricular interdependence: the fibrotic, non-compliant pericardium fixes total intracardiac volume, such that inspiration-related augmentation of right ventricular filling occurs at the direct expense of left ventricular filling (as the pulmonary veins are intrathoracic and not much gradient is produced during inspiration). The resultant discordant ventricular pressure changes, reduced myocardial stretch due to pericardial strain, with rapid y descent and an exaggerated x descent on waveforms, constitute the constrictive hemodynamic phenotype. Kussmaul sign (paradoxical rise or failure of decline in jugular venous pressure with inspiration) is a sign of impaired right heart function due to pericardial constraint. In restrictive cardiomyopathy, ventricular interdependence is absent: there is an intrinsic impairment of the myocardium, both ventricles share equally in the impaired ventricular relaxation, and respiratory variation in filling pressures is concordant. Pericardial thickening on CT does not confirm constriction, just as normal pericardial thickness does not exclude it. Multimodality integration combining cardiac MRI, CT-measured thickness, and invasive catheterization in equivocal cases remains the unequivocal diagnostic standard.
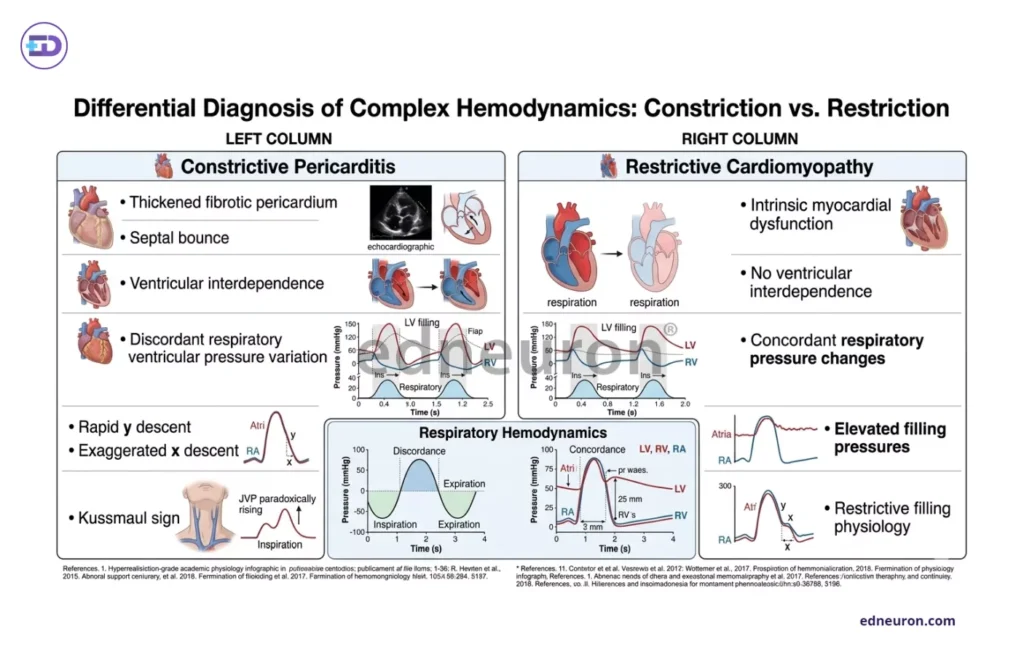
Fig 3 : Comparative study of Constrictive Vs Restrictive Physiology.
Conclusion
Pericarditis, by definition, is no longer a diagnosis of solely pericardial friction rub or identifying diffuse ST-segment elevation on ECG, but rather the task unravels the determination of finding whether inflammation is truly active, clinically meaningful, and therapeutically actionable. To reach such a destination requires assiduous integration of clinical probability, biomarker kinetics, and multimodality imaging in proportions as and when demanded by the clinical scenario. The 2025 ACC framework represents a genuine reflection astute strategy, but it simultaneously exposes the depth of the unresolved dichotomies and dilemmas that had rooted itself in this field for decades: the interpretive value of MRI-visible inflammation without symptoms, the immunological distinction between disease modification and potent suppression with IL-1 blockade, the subtleties between pericardial constriction vs myocardial restriction, and guidance, on how and when colchicine/corticosteroid de-escalation is deemed right something that warrants or demands the need for a validated inflammatory quiscence period determination. Some clarifications have been made, but these dilemmas persist like skin that refuses to be scaled.
References
- Adler Y, Charron P, Imazio M, et al. ESC Scientific Document Group. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015 Nov 7;36(42):2921-2964. PMID: 26320112.
- Wang TKM, Klein AL, Cremer PC, et al. 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Diagnosis and Management of Pericarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2025 Dec 23;86(25):2691-2719. PMID: 40767817.
- Gianni F., Solbiati M.; Gruppo di Autoformazione Metodologica (GrAM). Colchicine is safe and effective for secondary prevention of recurrent pericarditis. Intern Emerg Med. 2012 Apr;7(2):181-2. PMID: 22430920.
- Imazio M, Klein AL, Brucato A, et al. RHAPSODY Investigators. Sustained Pericarditis Recurrence Risk Reduction With Long-Term Rilonacept. J Am Heart Assoc. 2024 Mar 19;13(6):e032516. PMID: 38471825.
- Brucato A, Imazio M, Gattorno M, et al. Effect of Anakinra on Recurrent Pericarditis Among Patients With Colchicine Resistance and Corticosteroid Dependence: The AIRTRIP Randomized Clinical Trial. JAMA. 2016 Nov 8;316(18):1906-1912. PMID: 27825009.
- Geske JB, Anavekar NS, Nishimura RA, Oh JK, Gersh BJ. Differentiation of Constriction and Restriction: Complex Cardiovascular Hemodynamics. J Am Coll Cardiol. 2016 Nov 29;68(21):2329-2347. PMID: 27884252.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



