

Introduction
As a clinician, one can undeniably say that acute chest pain remains, perhaps, the most encountered and consequential diagnostic dilemma in clinical medicine. The institutional architecture ties the classic symptoms of retrosternal pain, diaphoresis, and ST elevation to myocardial infarction, especially when a physician works under highly stressful conditions, presented with an acute chest presentation, urging for prompt decision-making. But this embeds the risk for misclassification of a convergent species of mechanistically distinct pathology- acute myocarditis. What is peculiar is the ability of acute myocarditis to replicate the biochemical signature of infarction with such fidelity that it puts confidence in dicey waters. This ambiguity proves costly: overinvestigation with CT angiography not only heralds procedural risk but also the psychological burden that waits like a wolf for its patient, and, conversely, dwarfs the grave mortality of missed infarctions. Therefore, understanding how two distinct cardiac pathologies converge into an almost replicable phenotype is not only a matter of academic discussion but also of clinical necessity.
Pathophysiology
Myocardial infarction, a widely studied condition, is not scarce in the literature on its mechanisms. It arises from a ruptured atherosclerotic plaque, either within the coronary artery or embolising to it, occluding the artery and precipitating thrombosis, after which the myocardium suffers necrosis. Topographically, one can intuitively arrive at the fact that the occlusion will give rise to anatomically localized ischemic injury (although certain etiologies do cause diffuse MI)By contrast, myocarditis, as its name suggests, is an inflammatory sequelae of mostly viral etiologies (Coxsackievirus A/B, Parvovirus B19, adenovirus, echovirus, and COVID-19). Costantini M et al. (2011) report that 95% of patients admitted with presumptive myocarditis mimicking MI had flu-like prodromal symptoms of acute viral infection. These viruses have a predilection for males- increased testosterone levels cause enhanced myocyte and endothelial expression of receptors, facilitating entry of these viruses. The immune-mediated cascade injures myocytes more architecturally in the mid-myocardial and epicardial layers, with cellular infiltration. Myocarditis, which is non-ischemic in nature, can often translate to dilated cardiomyopathies or arrhythmias. Such a translation to chronic conditions is not clearly understood. As we notice the similarity of molecular cell injury, it is not surprising that diagnostically, such variable diseases arrive at the same biochemical signal- the release of troponins, proteins responsible for cardiac muscle contractility.
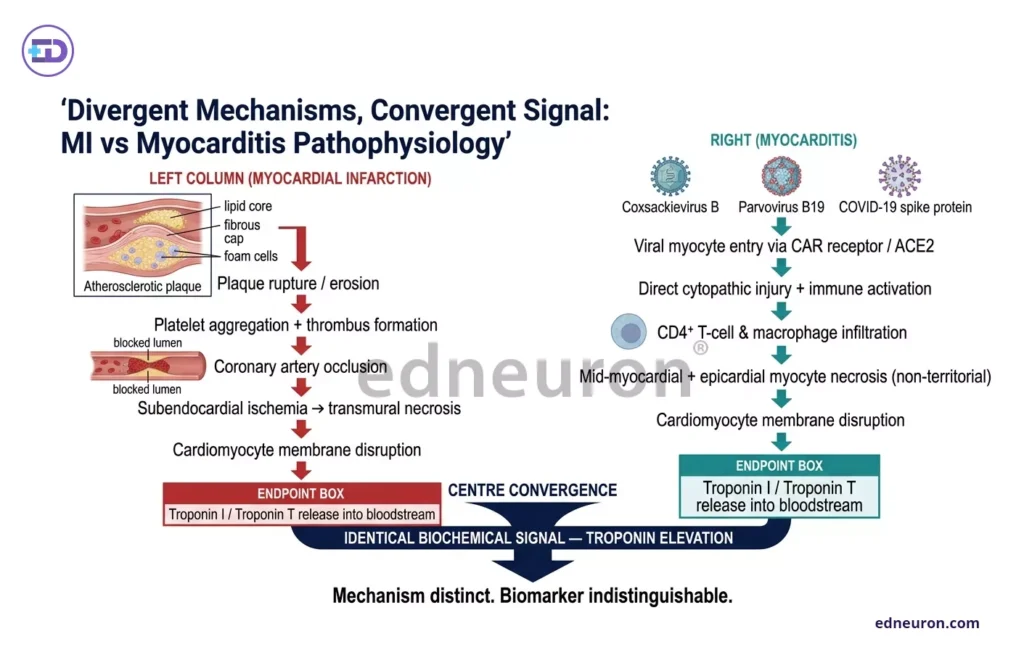
Fig 1: Pathophysiology from distinct etiologies converges at a single biomarker- elevation in troponin.
Diagnostic Modalities that Differentiate
With highly sensitive troponin assays, levels increase regardless of the mechanism, reflecting myocyte injury. In myocardial infarction, ischemia leads to necrosis, whereas myocarditis causes direct injury through inflammation. Markers like CRP, ESR, and CK-MB, although suggestive, tell us that some inflammatory process is in action, but:
- They don’t localize the process
- They don’t distinguish myocarditis from infarction reliably
- They can be elevated in infections, systemic inflammation, trauma, etc.
Zhang T et al. (2015) describe a case report of a 22-year-old male with retrosternal pain, elevated cardiac markers, and ECG ST-T changes, which led to an original misdiagnosis of acute myocardial infarction. When the patient was investigated with CT angiography, the coronary arterial tree was found to be completely normal. Eventually, a successful diagnosis was made based on prodromal symptoms of fever, rash, and flu, and the condition resolved within 2 weeks with antivirals and myoprotective therapy.
On Echocardiography: Myocarditis, resulting from global inflammation, leads to overall decreased ventricular function with reduced ejection fraction. MI, which more often than not is a localized ischemic attack, exhibits wall motion abnormalities; considerable overlap does exist, particularly when myocarditis is focal or when infarction involves diffuse territory.
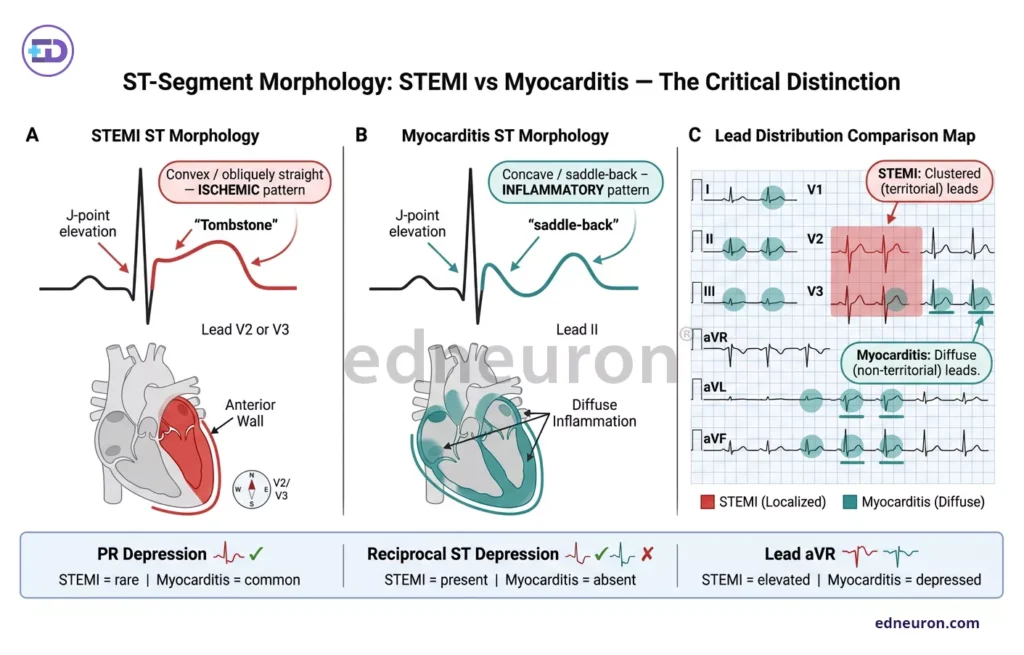
Fig 2: Comparative panel of ECG changes in MI vs Myocarditis
.
It is indeed cardiac magnetic resonance imaging (CMR) that has proven itself as the tenet of diagnostic tech used to differentiate when other modalities produce overlapping results. When other modalities ask, “Is the heart injured?” CMR provides the answer to “what kind of injury has the heart suffered?”
The Lake Louise criteria (2009) were updated in 2018 to incorporate T1 and T2 parametric mapping. CMR doesn’t just indicate the presence of injury; it also focuses on tissue characterization. The updated criteria demonstrate a sensitivity of 87.5% and a specificity of 96.2% for myocarditis, compared with 72.5% sensitivity under the original criteria.
- T1 mapping detects fibrosis and injury
- T2 mapping detects edema (active inflammation)
On CMR with contrast (late gadolinium enhancement):
- MI → subendocardial or transmural pattern
- Myocarditis → patchy, mid-wall/epicardial pattern
Endomyocardial biopsy remains the histological gold standard– it confirms lymphocytic infiltration and myocyte necrosis. Still, because it is invasive in nature, which comes with sampling error and operator dependence, its routine application is limited. CMR has, in practice, assumed the role of definitive non-invasive judge in the majority of cases.
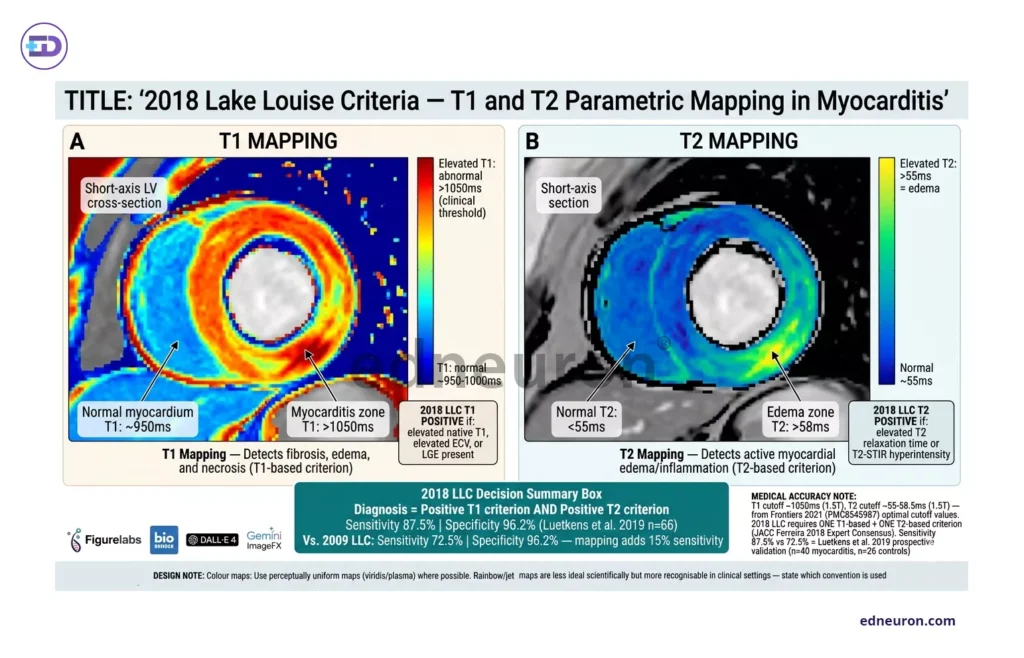
Fig 2: Diagnosis in myocarditis- Lake Louise criteria.
The Diagnostic Gray Zone (MINOCA as Differential)
MINOCA- Myocardial Infarction with Non-Obstructive Coronary Artery, as its name suggests, produces the same aberrant cardiac markers, ST changes as MI, but on CT angiography shows non-significant coronary arteries (<50%). It then becomes the failure of our binary thinking of MI vs not MI, and brings a paradigm shift to more mechanism-based thinking. It is not a final diagnosis but a working label; if not MI, then what? The diagnostic gray zone is perhaps most vividly inhabited by MINOCA: myocardial infarction with non-obstructive coronary arteries-a syndrome defined by troponin elevation and chest pain in the absence of flow-limiting coronary disease on angiography. Myocarditis accounts for between 9% and 22% of MINOCA presentations, and CMR identifies myocarditis in approximately 30% of this population (Mileva, N, Paolisso, P, Gallinoro, E., et al). We noticed that patients catheterized had normal coronaries, especially the younger male population, and those not catheterized harbored a risk of missed MI. Weighing the procedural risk against the benefit of accurately diagnosing MI, it is imperative in a hospital setting that when a young patient arrives with post-viral acute chest pain, the psychological burden of diagnostic uncertainty and overinvestigation risk in patients who might not need it in hindsight must employ serious deliberation. Conversely, an older patient with a genuine infarction misclassified as myocarditis based on an inflammatory history risks delayed reperfusion, with mortality consequences that outweigh the procedural risk of the catheterization withheld.
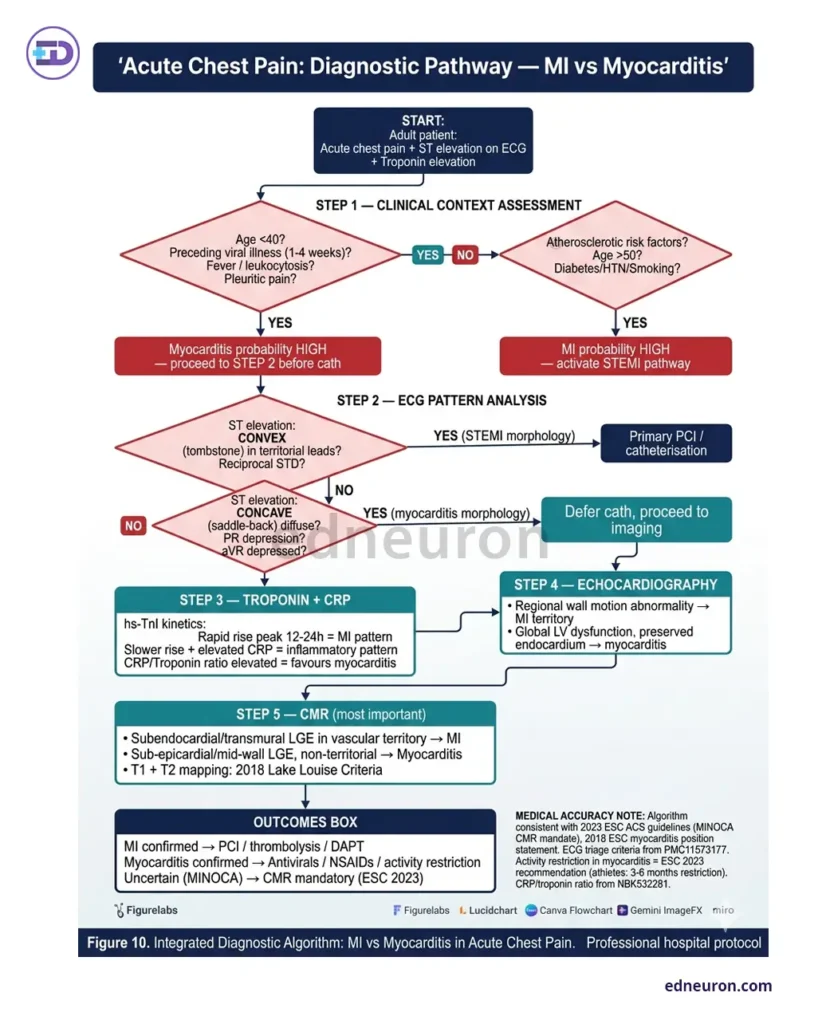
Fig 3: Stepwise evaluation strategy.
Conclusion
This article aims to illuminate the diagnostic reasoning and the caution of tying signs and diagnostic signals to a specific disease. Elevated troponin does not always indicate infarction, and ST-segment elevation does not necessarily imply plaque rupture. These are calls for help of tissue architecture and myocyte injury that various etiologies ultimately culminate in. It is thus a clinician’s duty to reconstruct the whole scenario, contextualize it within the patient portfolio, and produce such precision in making the diagnosis.
References
- Van Nierop J, Limburg A, van Ofwegen-Hanekamp CEE. Myocarditis mimicking acute myocardial infarction. Neth Heart J. 2015 Sep PMID: 26178204.
- Thilakaratne D, Bista R, Zenker M et al. Diagnostic Modalities and Treatment Options. Cureus. 2025 Mar PMID: 40034418.
- Potter JM, Hickman PE, Cullen L. Troponins in myocardial infarction and injury. Aust Prescr. 2022 Apr PMID: 35592367.
- Crisci G, Bobbio E, Gentile P et al. Biomarkers in Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Updated Review of the Literature. J Clin Med. 2023 Nov PMID: 38068265.
- Costantini M, Oreto G, Albanese A et al. Presumptive myocarditis with ST-Elevation myocardial infarction presentation in young males as a new syndrome. Clinical significance and long term follow up. Cardiovasc Ultrasound. 2011 Jan PMID: 21244654.
- Zhang T, Miao W, Wang S, Wei M, Su G, Li Z. Acute myocarditis mimicking ST-elevation myocardial infarction: A case report and review of the literature. Exp Ther Med. 2015 Aug PMID: 26622337.
- Luetkens JA, Faron A, Isaak A et al. Comparison of Original and 2018 Lake Louise Criteria for Diagnosis of Acute Myocarditis: Results of a Validation Cohort. Radiol Cardiothorac Imaging. 2019 Jul PMID: 33778510.
- Mileva, N, Paolisso, P, Gallinoro, E. et al. Diagnostic and Prognostic Role of Cardiac Magnetic Resonance in MINOCA: Systematic Review and Meta-Analysis. J Am Coll Cardiol Img. 2023 Mar, 16 (3) 376–389.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



