Introduction
Multiple myeloma, an age-dependent plasma cell disorder, often with increased prevalence in those aged >60 years, is a monoclonal light-chain gammopathy characterized by unbridled proliferation of plasma cells in the bone marrow, with a premalignant stage that initially presents as monoclonal gammopathy of undetermined significance (MGUS). Multiple myeloma accounts for more than 35000 estimated new cases and 12590 deaths annually (Siegel RL et al. 2023). MGUS is the precursor lesion of multiple myeloma, with a prevalence almost two-fold in black ethnicity. Unlike plasma cells, MM cells have a slow growth rate, so their progression to malignancy is about 1% per year. MM is associated with end-organ damage presenting as the classical tetrad of CRAB: Calcium elevation, Renal impairment, Anemia, and Bone lesions.
A retrospective analysis from the Mayo Clinic demonstrated that patients with MM experience a median diagnostic interval of over six months from symptom onset – a period during which irreversible end-organ damage with tissue impairment accumulates silently. Clinically, this diagnostic delay matters more than is often appreciated. Also, the quintessential CRAB lesions are often mislabeled by clinicians as follows:
- Bone pain- degenerative disease
- Anemia- anemia of chronic disease
- Renal impairment- diabetic nephropathy
Such clinical traps delay diagnosis and worsen prognosis. The CRAB acronym – formalized by the International Myeloma Working Group (IMWG) in 2003 and remains the anchor for identifying end-organ damage attributable to myeloma. In 2014, the IMWG revised the diagnostic criteria to include three additional biomarkers – collectively termed SLiM – that allow diagnosis before CRAB features develop, thereby enabling treatment, especially for patients with high progression risk factors. The present case illustrates MM diagnosis, a framework for examining pathophysiology, differential diagnosis, and staging.

Fig 1: The global burden representing the estimated no. of new cases and deaths.
Pathophysiology
Multiple myeloma originates from a post-germinal center B-cell that undergoes malignant transformation, acquiring oncogenic mutations, most commonly involving the immunoglobulin heavy chain (IgH) locus on chromosome 14q32 (IgH translocations and hypermutations), thereby activating oncogenes that confer a proliferative advantage and reduce the cellular drive of apoptosis. These MM cells are responsible for the exorbitant production of light chains: Bence-Jones proteins. The bone microenvironment plays a complex role that allows dynamic interactions: clonal plasma cells adhere to stromal cells via VLA-4/VCAM-1 and CD44/hyaluronan interactions. The autocrine and paracrine cytokine loops involving IL-6, VEGF, and IGF-1 dysbalance osteogenesis and osteoclastic activity, along with humoral and cellular deficiencies. This disruption in the bone homeostasis is central to the underlying CRAB tetrad. Myeloma cells secrete receptor activator of nuclear factor-κB ligand (RANKL) and macrophage inflammatory protein-1 alpha (MIP-1α), which, via osteoblasts, activate osteoclasts while simultaneously suppressing osteoblasts by DKK-1 and sclerostin. This overt activity of osteoclasts produces the characteristic lytic lesions observed in the patients at diagnosis. It is unlike any metastatic bone disease wherein there exist aberrant cycles of lysis and sclerosis; MM, conversely, is decompensated, and the lytic lesions predominate. Now, because osteoclast activation results in skeletal bone resorption, serum calcium levels far exceed those that the kidneys can adequately excrete. Moreover, this is compounded by already impaired tubules in MM patients due to cast obstruction (Tamm-Horsfall complexes) and light chain toxicity, inciting an inflammatory response. The pathophysiology here is not PTH-mediated, a distinction critical for ruling out primary hyperparathyroidism, but rather PTHrP (PTH-related peptide)-independent osteoclast activation. Hypercalcemia and NSAIDs, a drug this patient was taking, synergistically worsen GFR. In practice, this multi-hit renal injury means that even modest improvements in hydration and paraprotein control can produce meaningful GFR recovery, which distinguishes myeloma nephropathy from most other causes of advanced CKD.
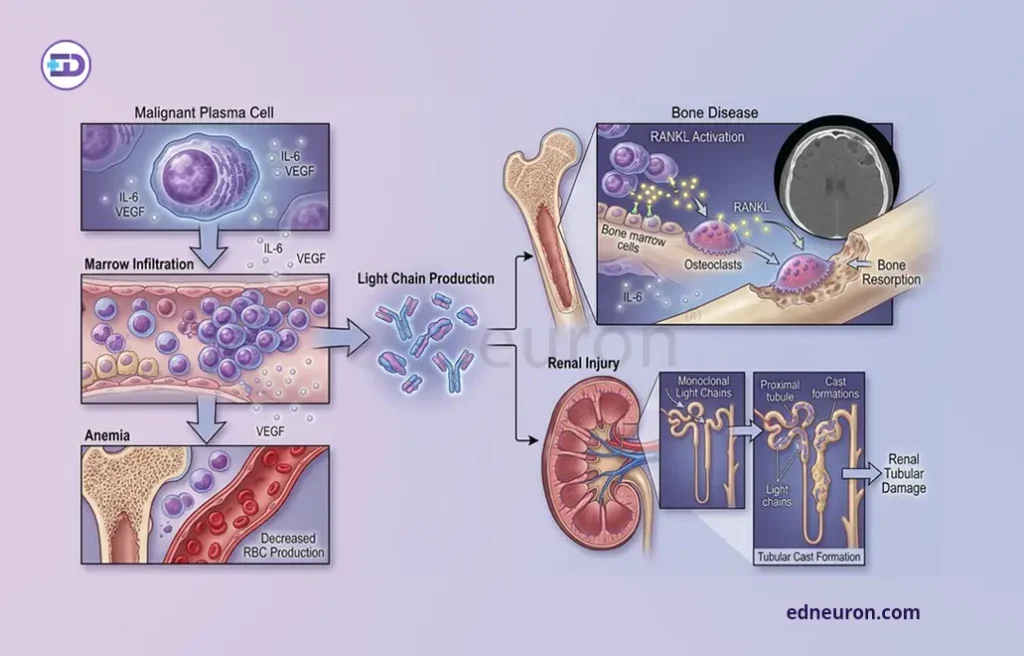
Fig 2: Malignant plasma cells secreting RANK ligand cause osteolytic lesions along with monoclonal light chain-mediated tubular damage.
Case Presentation
A 68-year-old retired schoolteacher presented to the hematology outpatient department with a six-month history of worsening lumbar pain unresponsive to NSAIDs, progressive exertional fatigue, and one episode of macroscopic haematuria. He had no prior malignancy, no family history of haematologic disease, and was a non-smoker. His comorbidities included well-controlled hypertension and type 2 diabetes mellitus (HbA1c 7.1%).
Examination findings: Vital signs were stable. He was notably pallid with conjunctival pallor. There was no lymphadenopathy, hepatosplenomegaly, or peripheral edema. GCS- Normal. Laboratory investigations: A full blood count revealed hemoglobin 8.1 g/dL (normocytic, normochromic), white cell count 5.8 × 10^9/L, and platelets 174 × 10^9/L. Serum analysis showed calcium 11.8 mg/dL, creatinine 2.6 mg/dL, eGFR 22 mL/min/1.73 m2, and albumin 2.9 g/dL. Beta-2 microglobulin was 7.4 mg/L. Serum protein electrophoresis (SPEP) demonstrated a discrete M-spike of 4.2 g/dL in the gamma region (refer to image below).
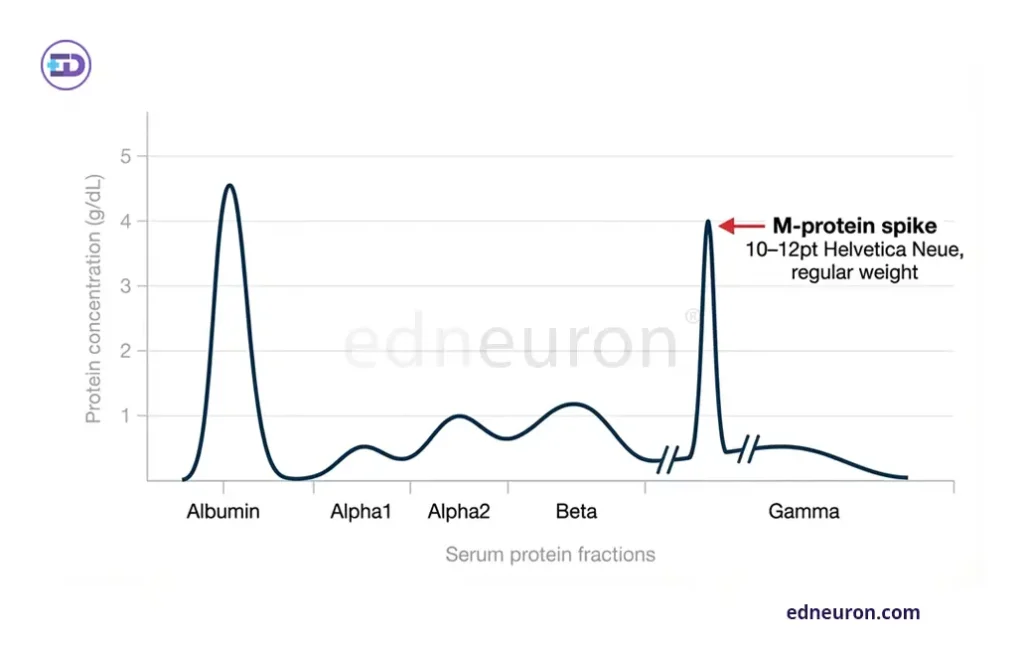
Fig 3: Serum electrophoresis showing M-spike on protein fractionation.
Serum immunofixation confirmed IgG kappa paraprotein. The serum free light chain ratio (kappa: lambda) was 148:1 (kappa 890 mg/L). 24-hour urine protein electrophoresis showed Bence-Jones proteinuria of 1.8 g/day.
Imaging: Plain radiograph skeletal survey demonstrated multiple punched-out lytic lesions of the skull vault (“pepper-pot” calvarium) (refer to the X-ray below).
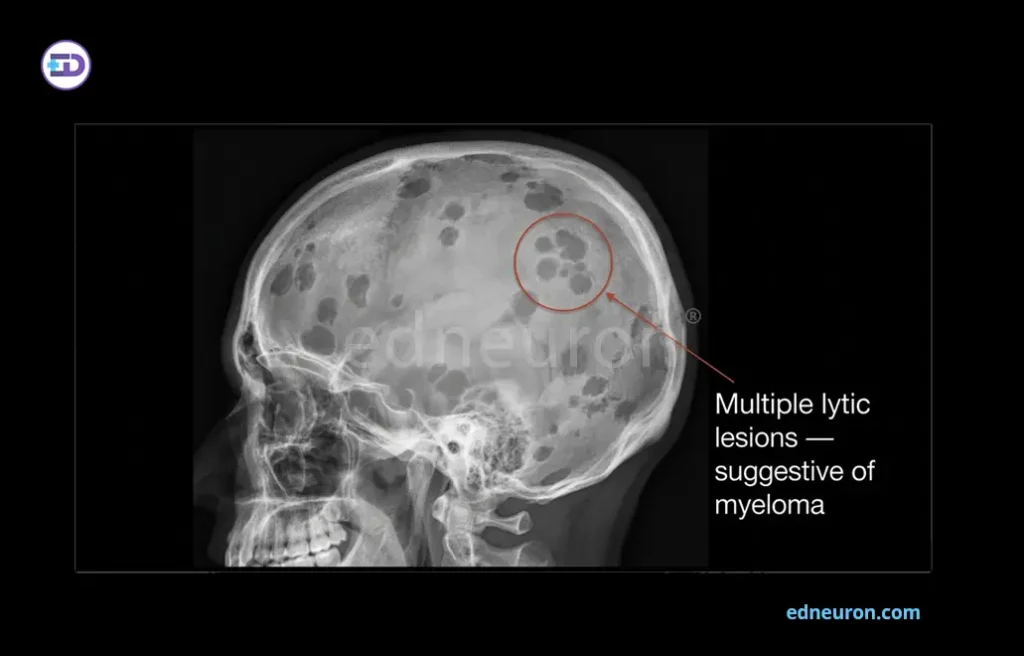
Fig 4: Skull X-Ray showing multiple osteolytic lesions.
Biopsy: Bilateral posterior iliac crest trephine biopsy revealed a markedly hypercellular marrow with 72% infiltration by atypical plasma cells, confirmed as clonal on immunohistochemistry (CD138+, CD38+, CD56+, kappa-restricted). Cytogenetic analysis by fluorescence in situ hybridization (FISH) demonstrated t(4;14)(p16;q32), a high-risk abnormality associated with FGFR3 dysregulation. No del(17p) or t(14;16) was identified. In summary, this patient satisfied all four CRAB criteria simultaneously, a clinical presentation that underscores how advanced end-organ damage had accumulated over the six-month diagnostic interval.
Differential Diagnosis
- Metastatic bone disease, worthy of being a differential, is ruled in by the clinician due to coinciding bone pain presentation. However, unlike any metastatic lesion in bone, which is marked by haphazard lysis, sclerosis, and periosteal reaction, MM exhibits only lytic bony characterization. The M-spike on SPEP, the markedly elevated free light chain ratio, and the bone marrow biopsy result are definitive.
- Waldenström macroglobulinemia (WM) is a plasma cell lymphoma producing IgM paraprotein. Unlike MM, WM rarely causes bone disease and typically presents with lymphadenopathy, splenomegaly, and hyperviscosity syndrome rather than CRAB features. IgM paraprotein on immunofixation should prompt consideration of WM. In this case, the IgG kappa paraprotein and bone marrow showing plasma cell predominance rather than lymphoplasmacytic infiltrate, then exclude WM.
- Monoclonal gammopathy of undetermined significance (MGUS) and smoldering myeloma (SMM) represent the earlier, pre-malignant stages of the same clonal spectrum. Critically, MGUS and SMM are defined when the monoclonal protein is < 30 g/1 and the bone marrow clonal cells are < 10% with no evidence of multiple myeloma, other B-cell proliferative disorders, or amyloidosis. In asymptomatic (smoldering) myeloma, the M-protein is ≥ 30 g/L and bone marrow clonal cells are≥ 10%, with no related end-organ damage. This patient’s renal impairment, anemia, hypercalcemia, bone lesions, and 72% bone marrow plasma cell infiltration exclude both diagnoses unambiguously.
Diagnostic Criteria
IMWG 2014 (Revised SLiM-CRAB) -The revised criteria require both of the following:
- ≥10% clonal bone marrow plasma cells or biopsy-proven plasmacytoma; AND
- At least one myeloma-defining event: either a CRAB feature OR one of the SLiM biomarkers: ≥60% clonal bone marrow plasma cells; free light chain ratio ≥100 with involved FLC ≥100 mg/L; or ≥2 focal lesions on MRI (each ≥5 mm in diameter).
In practice, this distinction is critical because it means that a patient with 65% bone marrow plasma cells but no CRAB features now meets criteria for active myeloma and warrants treatment – a paradigm shift from the pre-2014 ‘watch-and-wait’ approach. This patient meets all four CRAB criteria and has 72% plasma cell infiltration, thereby fulfilling the diagnostic criteria on multiple independent criteria simultaneously.
Staging

Table 1: Standard risk factors for MM (reference: Antonio Palumbo et al.)
MM: multiple myeloma, ISS: International Staging System, CA: chromosomal abnormalities, iFISH: interphase Fluorescence in Situ Hybridization, LDH: Lactate Dehydrogenase, R-ISS: revised International Staging System. This patient is R-ISS Stage III — the highest-risk category.
Conclusion
This case illustrates three imperatives that define optimal myeloma care. First, CRAB recognition must be systematic and reflexive: each of the four features in this patient had a plausible, common alternative explanation-degenerative spinal disease, diabetic nephropathy, anemia of chronic disease, and age-related hypercalcemia, yet their co-occurrence in an elderly patient mandated an immediate myeloma workup. In practice, this often means ordering SPEP and serum free light chains in any patient over age 50 with unexplained anemia, renal impairment, or bone pain – a simple step that substantially shortens the diagnostic interval. Second, the 2014 IMWG SLiM-CRAB criteria have real clinical consequences. The inclusion of biomarker-defined disease, particularly ≥60% bone marrow plasma cells and FLC ratio ≥100 means that myeloma can now be diagnosed and treated before CRAB features develop. The SLiM criteria are not merely diagnostic footnotes; they represent a conceptual commitment to treating the highest-risk patients before the clock of organ damage has already advanced. Ultimately, multiple myeloma is a disease in which diagnostic delay is an avoidable tragedy.
References
- Rajkumar SV. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am J Hematol. 2022 Aug PMID: 35560063.
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48.
- Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21–33.
- The International Myeloma Working Group (2003), Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. British Journal of Haematology, 121: 749-757.
- Kuehl WM, Bergsagel PL. Molecular pathogenesis of multiple myeloma and its premalignant precursor. J Clin Invest. 2012 Oct PMID: 23023717.
- Nelson Leung, Frank Bridoux, Colin A et al. on behalf of the International Kidney and Monoclonal Gammopathy Research Group, Monoclonal gammopathy of renal significance: when MGUS is no longer undetermined or insignificant. Blood 2012; 120 (22): 4292–4295.
- Antonio Palumbo et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol 33, 2863-2869(2015).

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi