Introduction
The clinical management of acute leukemia (AL) has transitioned from a morphology-heavy paradigm to an integrated diagnostic framework where multiparametric flow cytometry (MFC) acts as the vital bridge between cellular phenotype and genetic architecture. While the French-American-British (FAB) system remains a descriptive anchor, it lacks the precision required for modern risk stratification. This review evaluates the clinical differences between acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL), focusing on immunophenotypic surrogacy, age-dependent risk factors, and the persistent challenge of detecting leukemic stem cells (LSCs).
Lineage Divergence and the Utility of Surrogate Markers
At the point of preliminary diagnosis, the primary goal is rapid lineage assignment to direct induction therapy. The standard relies on lineage-specific markers: myeloperoxidase (MPO) for AML, cCD79a for B-ALL, and cCD3 for T-ALL. However, the most critical clinical distinction often involves Acute Promyelocytic Leukemia (APL, M3), where the risk of fatal coagulopathy demands immediate recognition. Clinically, the combined absence of HLA-DR and CD34 remains the most robust surrogate marker for APL, effectively excluding non-APL AML subtypes that typically express these antigens.
In the context of ALL, “lineage infidelity,” i.e., the expression of myeloid antigens like CD13 or CD33, is frequently observed and carries distinct biological implications. In adolescent and young adult (AYA) patients, a population with suboptimal survival rates compared to children, aberrant expression of CD13 and CD33 is significantly associated with the Philadelphia chromosome [t(9;22)]. This suggests that MyAg-positive ALL may reflect a more primitive, “stem-like” biology that contributes to treatment resistance.
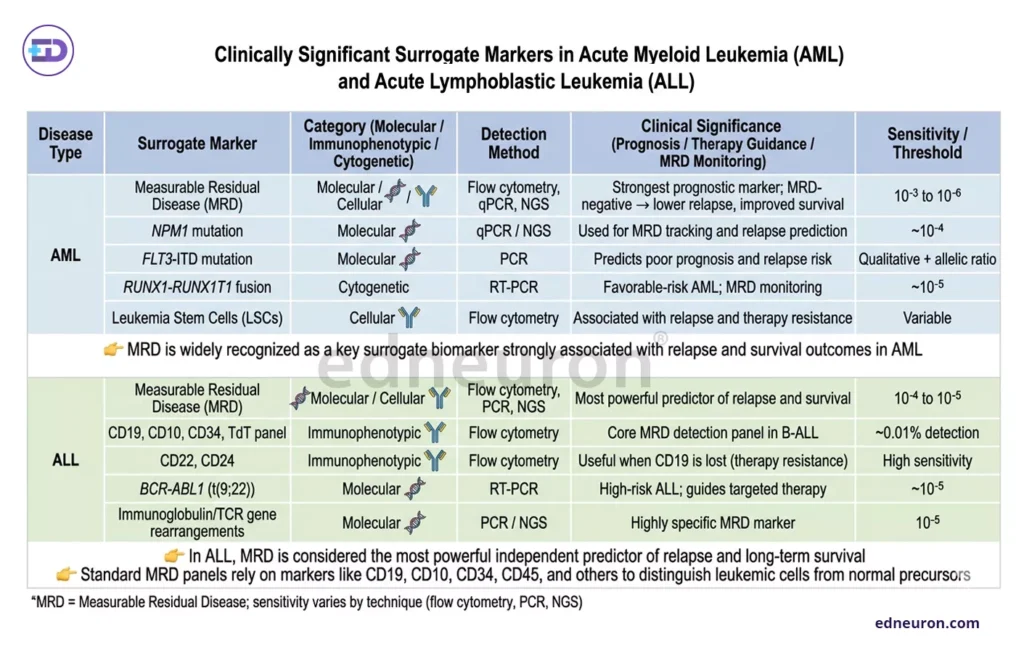
Fig 1: Key to icons: 🧬 = Molecular category; 🧬+Y = Molecular/Cellular category; Y = Cellular/Immunophenotypic category.
The Persistence Paradox: LSCs and Recurrence
Despite achieving morphological complete remission (CR), over 50% of AML patients relapse. This clinical failure is largely attributed to the persistence of leukemic stem cells (LSCs), which often reside within the CD34+/CD38− compartment. While MRD sensitivity in ALL often reaches <0.01%, AML MRD detection by conventional MFC is typically limited to ~0.1%. This “sensitivity gap” is problematic because LSCs possess unique properties of dormancy and drug resistance that allow them to evade standard cytotoxic regimens.
Clinically, the detection of LSCs using markers such as CD123, CD45RA, and TIM-3 provides superior prognostic value compared with blast-based MRD alone. Patients who remain LSC-positive post-induction, even if labeled MRD-negative, face a significantly higher risk of early relapse. This necessitates a shift toward high-sensitivity techniques, such as spectral flow cytometry, which enable distinguishing rare LSC clones from residual normal hematopoietic stem cells using 20+ parameters.
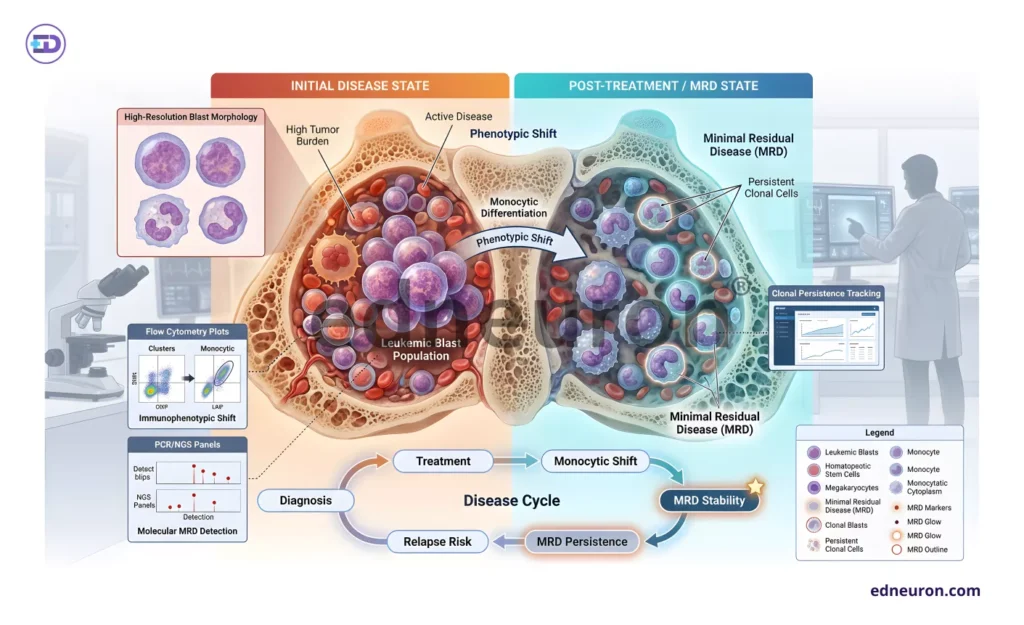
Fig 2: Diagrammatic comparison between the initial and post-treatment stage depicting the Monocyte shift and the occurrence of MRD stability.
The “Monocytic Shift” and MRD Stability
A significant diagnostic pitfall exists in DUX4-rearranged (DUX4r) B-ALL, a subtype that often undergoes a misleading “monocytic switch” or loses CD10 expression during induction therapy. This phenotypic plasticity can lead to false-negative results in traditional measurable residual disease (MRD) monitoring if clinicians rely solely on CD10/CD19 gating. Recent evidence highlights CD371 (CLL-1) as a highly stable marker for DUX4r B-ALL; unlike other markers, CD371 expression persists throughout therapy, providing a reliable anchor for tracking residual clones even when the primary blast gate shifts toward a monocytic phenotype.
Clinical Interpretation and Practical Implications
For the practicing clinician, these findings suggest that AL diagnosis should no longer be viewed as a static event. The potential for immunophenotypic shifts—whether through clonal evolution in AML or lineage switching in ALL—requires MRD strategies that account for marker instability. Furthermore, integrating artificial intelligence (AI) into flow data interpretation may soon reduce “subjective gating” errors that currently limit inter-laboratory consistency.
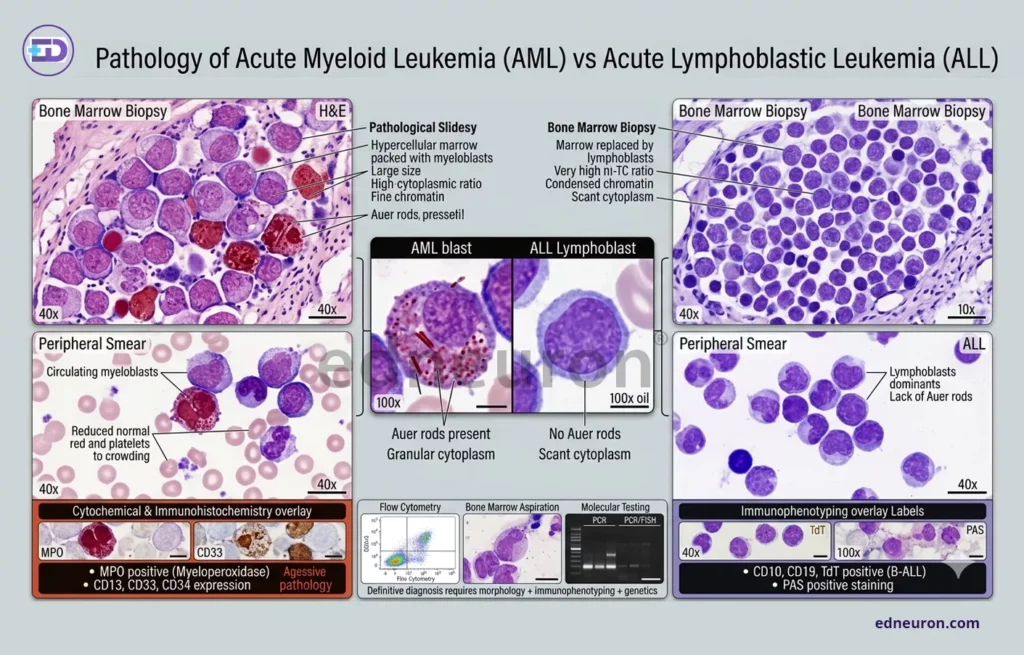
Fig 3: Pathological graphic presents a comprehensive visual and immunophenotypic analysis that distinguishes the morphological features of Acute Myeloid Leukemia (AML) from those of Acute Lymphoblastic Leukemia (ALL).
Limitations and Uncertainty
A primary limitation remains the cross-reactivity of immunophenotypic markers; no single antigen is entirely specific for malignancy. Additionally, while LSC monitoring is promising, much of the data is derived from intensive chemotherapy trials, and its relevance in the era of targeted agents (e.g., venetoclax) requires further prospective validation.
Conclusion
The clinical divergence between AML and ALL is increasingly defined by the stability of residual clones rather than initial lineage. Prioritizing stable surrogates like CD371 in B-ALL and quantifying the therapy-resistant LSC burden in AML are essential steps toward preventing the “avoidable tragedy” of late-stage relapse.
References
- Zhou Y, et al. Clinically useful flow cytometry approach to identify immunophenotype in acute leukemia. Medicine (Baltimore). 2019;98(2):e13917.
- Yadav V, Raveendranath V, Ganesan P, Kar R, Priyadharshini R, Manivannan P. Immunophenotypic characteristics and cytogenetic analysis of adolescent and young adult B-cell acute lymphoblastic leukemia. Cureus. 2024;16(9):e68735.
- Khoury JD, Solary E, Abla O, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms. Leukemia. 2022;36:1703–1719.
- Campo E, Jaffe ES, Cook JR, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia. 2022;36:1720–1748.
- Arber DA, Orazi A, Hasserjian R, et al. The WHO classification of haematolymphoid tumours: overview and principles. Leukemia. 2022.
- Kumar S, et al. Flow cytometry in acute myeloid leukemia and detection of minimal residual disease. Journal of Laboratory Physicians. 2024.
- Zhang X, et al. Flow cytometric detection of leukemic stem cells in acute myeloid leukemia. Frontiers in Pharmacology. 2025.
- Kern W, et al. The role of flow cytometry in the classification of myeloid disorders. Annals of Hematology. 2023.
- Sharma P, et al. Flow cytometric immunophenotypic profile of acute leukemia: a tertiary care center study. Indian Journal of Pathology and Microbiology. 2012;55(4):564–568.
- Béné MC, Castoldi G, Knapp W, et al. Proposals for the immunological classification of acute leukemias (EGIL classification). Leukemia. 1995;9(10):1783–1786.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India