

Introduction
Vitamin A (retinol) is a vital, fat-soluble nutrient needed for cell growth, immune function, and healthy vision. In wealthier countries, Vitamin A Deficiency (VAD) is rare, but it is still a major cause of preventable childhood blindness worldwide, especially in sub-Saharan Africa and Southeast Asia. The shift from mild deficiency to permanent eye damage highlights serious gaps in public health systems.
Pathophysiological Progression:
The Visual Cycle and Epithelial Decay
The main sign of VAD is usually night blindness, which occurs when the retina cannot produce enough visual pigment. Retinol is needed to form rhodopsin, and without it, the eyes cannot adjust to dim light.
If the body continues to lack vitamin A, usually when blood retinol drops below 20 μg/dL, the condition can progress to xerophthalmia. This includes several eye problems:
- Conjunctival Xerosis: This is when the white part of the eye becomes dry and loses its shine.
- Bitot’s Spots: These are foamy, triangle-shaped patches on the eye made up of hardened cells.
- Corneal Ulceration and Keratomalacia: In the most severe stage, the cornea breaks down and softens, leading to loss of shape and permanent blindness.
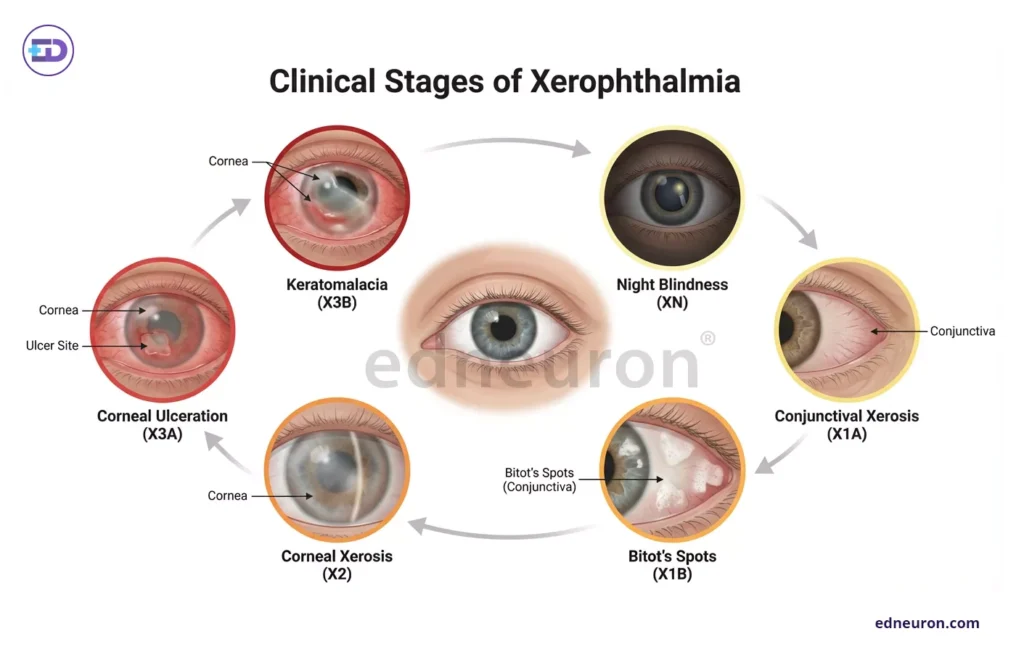
Fig 1: A diagrammatic cycle of the onset of Xerophthalmia and its various stages.
Clinical Data and Epidemiological Burden
Recent surveys in southwest Ethiopia indicate that this problem remains common. Out of 411 preschool children screened, 2.2% had clinical VAD, which is much higher than the World Health Organization’s threshold of 1.5% for public health concern.
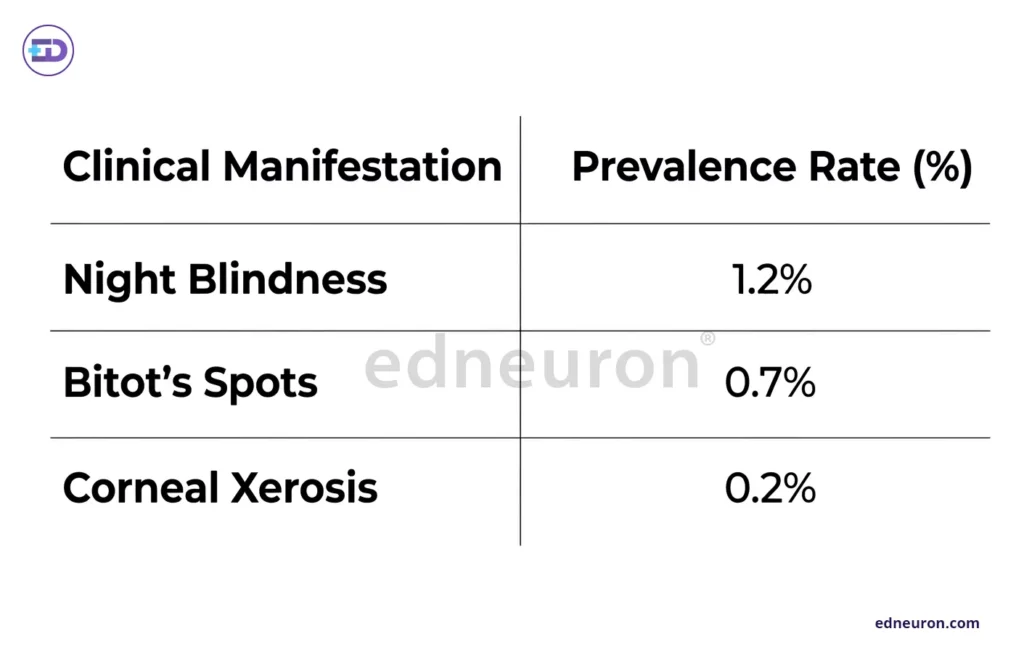
Table 1: Data source: Community-based survey in Cheha district.
Importantly, the risk of death is much higher for children who have both night blindness and Bitot’s spots. Their mortality rate is nine times greater than for those with only mild deficiency. This is often because their body’s protective barriers in the lungs and gut are weakened, making them more likely to get serious infections.
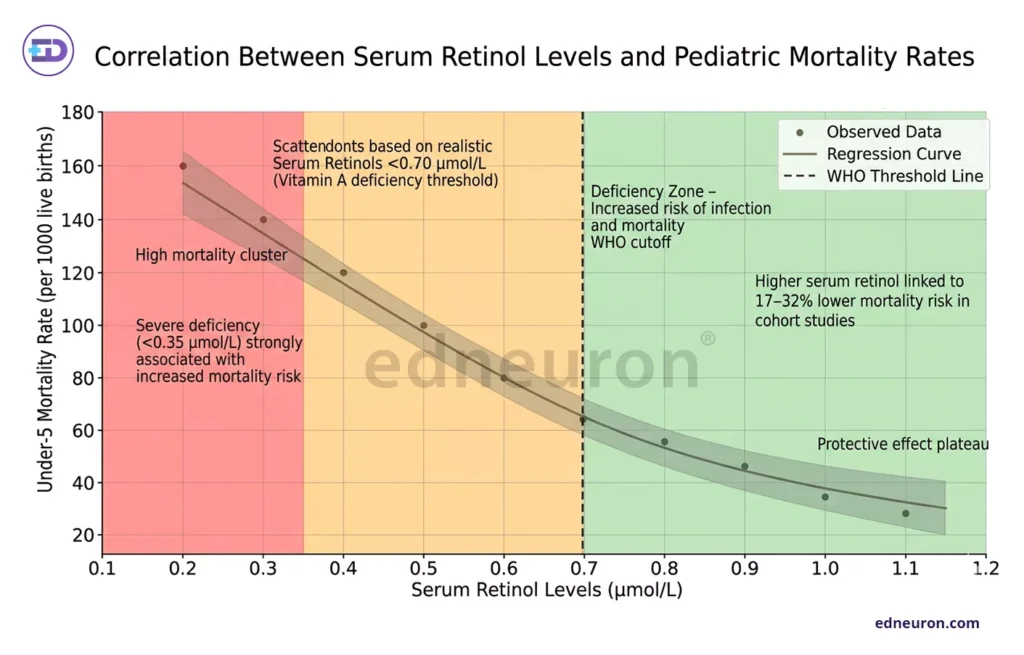
Fig 2: Correlation Between Serum Retinol Levels and Pediatric Mortality Rates (WHO Deficiency Threshold = 0.70 µmol/L)
Etiological Complexity:
Beyond Simple Malnutrition
While insufficient dietary intake of carotenoids (plant-based) or retinoids (animal-based) is the primary driver, secondary factors frequently exacerbate the condition. Measles infection is a known precipitator, capable of inducing a >30% drop in serum retinol levels due to rapid utilization and urinary excretion during the inflammatory response. In developed regions, VAD is almost exclusively secondary to malabsorptive pathologies, including inflammatory bowel disease (IBD), cystic fibrosis, or a history of bariatric surgery (e.g., biliopancreatic diversion).
Therapeutic Imperatives and Prevention
Treatment mainly involves giving high doses of vitamin A. The WHO recommends that children aged 6 to 59 months receive 200,000 IU every 4 to 6 months. For children with eye symptoms, three doses are given on Day 1, Day 2, and Week 2 to stop the cornea from breaking down. For long-term prevention, countries are turning to biofortified foods such as Golden Rice and orange-fleshed sweet potatoes to help at-risk groups obtain sufficient vitamin A from their diets.
Global Trends in Vitamin A Status
Vitamin A deficiency shows clear regional disparities. According to the World Health Organization, serum retinol levels below 20 μg/dL are most common in sub-Saharan Africa and South Asia, often affecting over 30% of children, while rates in North America and Western Europe are below 1%. Globally, prevalence has declined from about 33% in the 1990s to ~25% in recent years, driven by supplementation and fortification programs. However, progress remains uneven, with subclinical deficiency still widespread despite reductions in overt clinical disease.
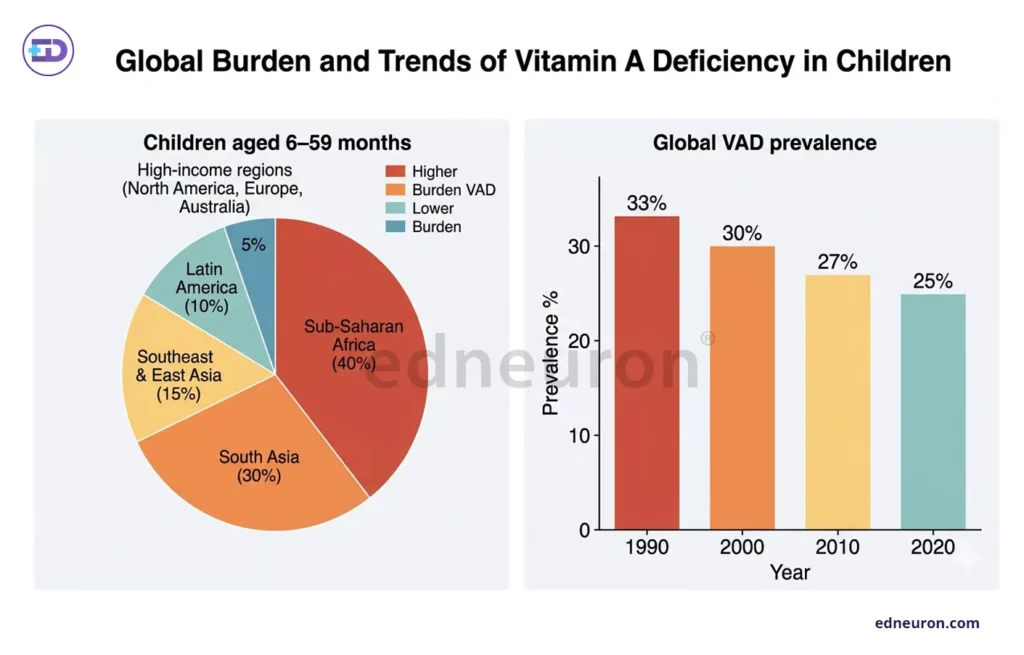
Fig 3: A pie and bar chart correlation between the prevalence of VAD in children and in the population over the last 3 decades.
Conclusion
Ultimately, the eradication of “national blindness” requires a transition from reactive clinical management to proactive, sustainable public health strategies. While acute Vitamin A Supplementation (VAS) remains the immediate priority, achieving long-term ocular stability requires integrating biofortified crops such as Golden Rice and orange-fleshed sweet potatoes into regional food systems, thereby effectively reducing the odds of clinical VAD by 81%. Furthermore, maximizing Antenatal Care (ANC) utilization is a vital predictor of success, as maternal nutritional counseling is associated with a 89% reduction in pediatric VAD risk. By maintaining high clinical vigilance for early indicators like nyctalopia and addressing the subclinical “tip of the iceberg,” the medical community can prevent the catastrophic mucosal decay and high pediatric mortality rates that define this preventable crisis.
References
- Sinha, D., et al. (2023). Vitamin A deficiency compromises the barrier function of the retinal pigment epithelium. PNAS Nexus. Advance online publication.
- Siddiqui, W. J., & Reddy, V. (2024). Vitamin A deficiency/

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India


