Introduction
The clinical management of congenital heart disease (CHD) has been revolutionized by echocardiographic precision and advanced surgical techniques, and yet a persistent diagnostic blind spot remains at the intersection of hematology and hemodynamics. While we categorially divide defects into cyanotic and acyanotic based on the presence of right-to-left shunts, this binary fails to capture the dynamic physiological adaptations or failures occurring within the patient’s oxygen transport system. The central clinical tension lies in the deceptive nature of hemoglobin levels in the hypoxic environment; what appears “normal” by conventional standards may actually represent a state of relative anemia, masking a profound risk for postoperative failure.
This raises a fundamental question:
Are we systematically underdiagnosing and under-treating a critical driver of surgical morbidity by adhering to obsolete hematological thresholds?
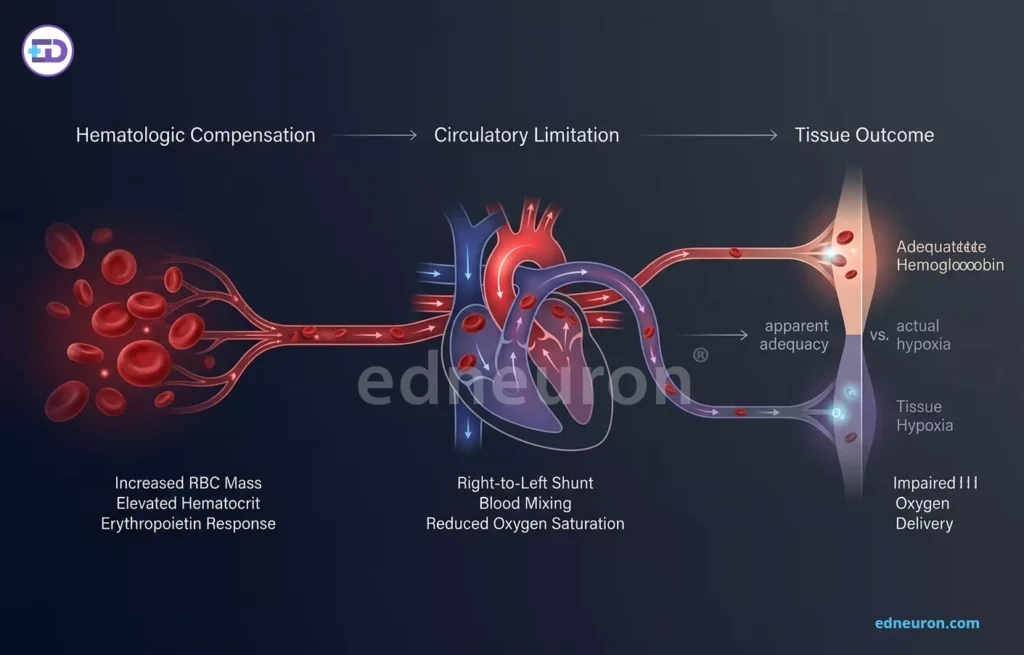
Fig 1: Hematologic compensation via increased RBS mass masks tissue hypoxia caused by circulatory limitations in cyanotic pediatric CHD
The Illusion of Secondary Erythrocytosis
In the cyanotic patient, chronic hypoxemia triggers a compensatory surge in erythropoietin, driving secondary erythrocytosis to preserve arterial oxygen content (CaO2). This physiological pivot creates a diagnostic mirage where actual hemoglobin (Hb) concentrations rarely fall below the age-adjusted lower limit of normal, with one study identifying such “absolute” anemia in only 4.5% of cyanotic children. However, the reality of tissue oxygenation is more complex, as the severity of this compensatory response should be inversely proportional to resting oxygen saturation (SpO2). What emerges is not a simple deficiency but a failure of compensation; a patient who cannot mount a sufficient erythrocytic response to their degree of hypoxemia is effectively anemic, regardless of their absolute Hb number. When anemia is defined as the product of [Hb x SpO2], the prevalence of “relative” anemia jumps to 21.6%, revealing a significant cohort of patients who are physiologically ill-prepared for surgical stress.
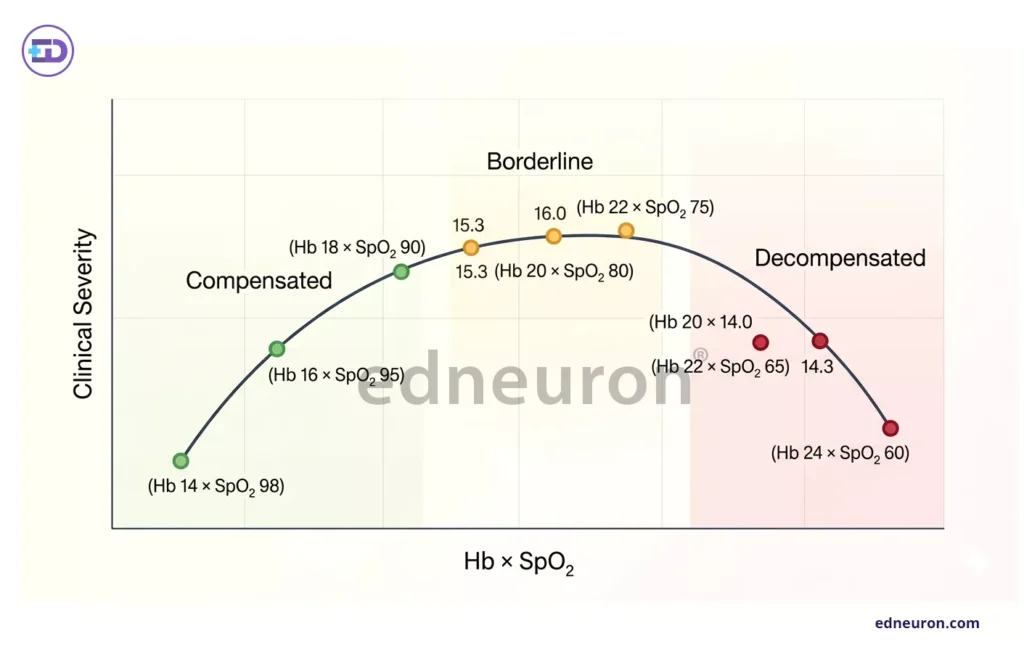
Fig 2: Clinical severity states in cyanotic pediatric CHD categorized by hemoglobin and oxygen saturation thresholds
The [ Hb x SpO2 ] Metric as a Prognostic Arbiter
The clinical utility of integrating Hb and SpO2 into a single prognostic marker is underscored by its strong correlation with surgical outcomes. Children whose compensation falls below age-adjusted limits (Hb x SpO2 < aaHb) face a significantly higher risk of in-hospital death, 12.5% compared to 4.6% in those with sufficient compensation. This suggests that the physiological cost of insufficient secondary erythrocytosis is not merely a laboratory curiosity but a primary driver of cardiac arrest, sepsis, and prolonged mechanical ventilation. What complicates this further is that the most vulnerable patients—those with transposition of the great arteries or duct-dependent lesions—often lack the time to mount an adequate compensatory response before urgent intervention is required. In these acute scenarios, the absence of high-altitude residence or long-standing cyanosis, which typically stimulates erythropoiesis, leaves the infant in a state of uncompensated “hemic frailty” at the very moment of maximum surgical stress.
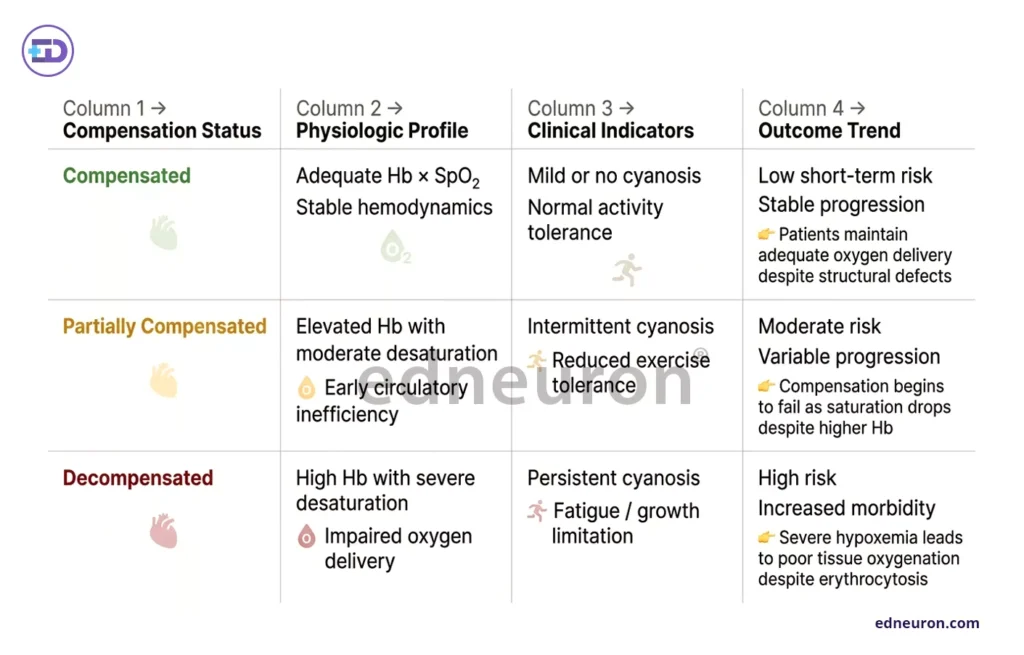
Fig 3: Classification of compensation status in pediatric cyanotic CHD based on clinical and physiological profiles
Clinical Outcomes and Developmental Confounding
While the diagnostic challenge is most acute in cyanotic CHD, acyanotic phenotypes are not exempt from hematological complexity. Anemia remains prevalent in 19.3% of acyanotic cases, often remaining asymptomatic and undiagnosed until the preoperative visit. A more plausible explanation for the systemic nature of these abnormalities may lie in shared developmental pathways. For instance, a notable correlation exists between Ventricular Septal Defects (VSD) and mild neutropenia, suggesting that solitary developmental factors may regulate both ventricular formation and hematological development during the embryonic period. This implies that the hematological profile of a CHD patient is not merely a consequence of their heart defect, but perhaps a parallel manifestation of the same underlying genetic or environmental insult.
Broader Perspectives and Social Determinants
Beyond the bench and the bedside, the outcome of CHD management is inextricably linked to the patient’s environment. Socioeconomic factors, including low family income and uneducated parental status, are significant risk factors that correlate with late diagnosis and poor nutritional status. Machine learning models, particularly artificial neural networks, have identified that factors such as a mother’s fast-food consumption and poor housing conditions are significant predictors of whether a child will present with cyanotic or acyanotic lesions. These variables act as distal drivers of the very physiological failures we see in the ICU, where poor prenatal nutrition likely limits the infant’s ability to mount the iron-dependent erythrocytic response necessary to survive cyanotic stress.
Conclusion
The diagnostic encounter at the CHD-hematology interface requires a departure from static laboratory ranges toward a dynamic assessment of oxygen-carrying capacity. Clinicians must recognize that in the cyanotic landscape, a “normal” hemoglobin is often a sign of failing compensation rather than health. Moving forward, integrating the Hb x SpO2 metric into preoperative risk stratification and addressing the socioeconomic determinants of “hemic frailty” will be essential for improving survival in these complex patients.
References
- Tsuda, T. (2016). Cyanotic congenital heart disease. Journal of Heart and Cardiology. Retrieved from ResearchGate.
- Mohammadi, M., et al. (2022). Hematological indices in children with acyanotic congenital heart disease. Egyptian Journal of Medical Human Genetics, 23, Article 262.
- Gupta, A., Abqari, S., Shahab, T., Rabbani, M. U., Ali, S. M., & Firdaus, U. (2024). Profile of acyanotic congenital heart defects. International Archives of Biomedical and Clinical Research, 2(4), 11–16.
- Rao, P. S. (2019). Management of congenital heart disease: State of the art—Part II: Cyanotic heart defects. Children, 6(4), 54.
- Zhou, D., Deng, L.-J., Ling, Y.-F., & Tang, M.-L. (2022). Preoperative hemoglobin level, oxygen saturation, and postoperative outcomes in children with cyanotic congenital heart disease: A propensity-score matching analysis. Frontiers in Pediatrics, 9, 762241.
- L., & Quek, S. C. (2025). Systematic review and network meta-analysis of outcomes of transcatheter strategies and surgical shunts for duct-dependent cyanotic congenital heart disease. Frontiers in Cardiovascular Medicine.
- Shahid, M., et al. (2024). Prediction of cyanotic and acyanotic congenital heart disease using machine learning models. World Journal of Clinical Pediatrics, 13(1).

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India