

Introduction
Post-Treatment Lyme Disease Syndrome (PTLDS) represents one of the most contested and hotly debated clinical entities in contemporary infectious disease. Lyme’s disease has now reached the pinnacle of ever-growing concern in the United States, and in 2019, it became the sixth most commonly notifiable disease, with almost 476,000 cases reported annually. 10-20% of patients who complete guideline-concordant antibiotic therapy for confirmed Lyme borreliosis develop PTLDS. It is something defined not by its mechanism, but by its persistence after adequate treatment. The patients with their disabling symptoms-fatigue, musculoskeletal pain, arthralgia, and neurocognitive impairment- endure for months to years without objective evidence of ongoing infection. It is this paradox that has perplexed the researchers since time immemorial. We do have plausible competing frameworks: residual or ongoing infection with Borrelia burgdorferi, immune dysregulation, post-infectious autoimmunity, and molecular mimicry with central nervous system sensitization; however, when these hypotheses are applied to explain the full clinical phenotype in isolation, they land in an utter conundrum. Their coexistence intriguingly reflects a failure to reconcile infection, immunity, and neurobiology into a unified explanatory model, and it is precisely that failure which defines the diagnostic and therapeutic impasse clinicians face.
Clinical Definition and Diagnostic Boundaries
PTLDS is operationally defined by four criteria:
- Documented and treated Lyme disease.
- Completion of recommended antibiotic therapy, depending on the stage of the infection. It can be anywhere from 10 days to 1 month of oral Doxycycline, with or without parental antibiotics.
- Onset of symptoms within six months of diagnosis, and persistence of those symptoms beyond six months after treatment, in the absence of an alternative explanation.
This exclusionary framework is structurally similar to other post-infectious syndromes, such as post-viral fatigue syndrome (PVFS), and even chronic active Epstein-Barr virus (CAEBV), which present with some overlapping symptoms. This identifies a specific population, perhaps with genetic susceptibilities, in which the absence of pathognomonic findings or conclusive seropositivity compounds the diagnostic challenge. Fatigue, musculoskeletal pain, and cognitive symptoms are non-specific; the diagnosis can only be made when there exists a definitive temporal relationship and exclusion. Two-tier serological testing, IFA/ ELISA followed by western immunoblot, the cornerstone of acute Lyme diagnosis, has limited utility in PTLDs because the IgG antibodies persist for years after the infection has cleared and cannot distinguish active from resolved disease. This essentially creates a vacuum in which clinical reasoning must shoulder the disproportionate burden of making a diagnosis.
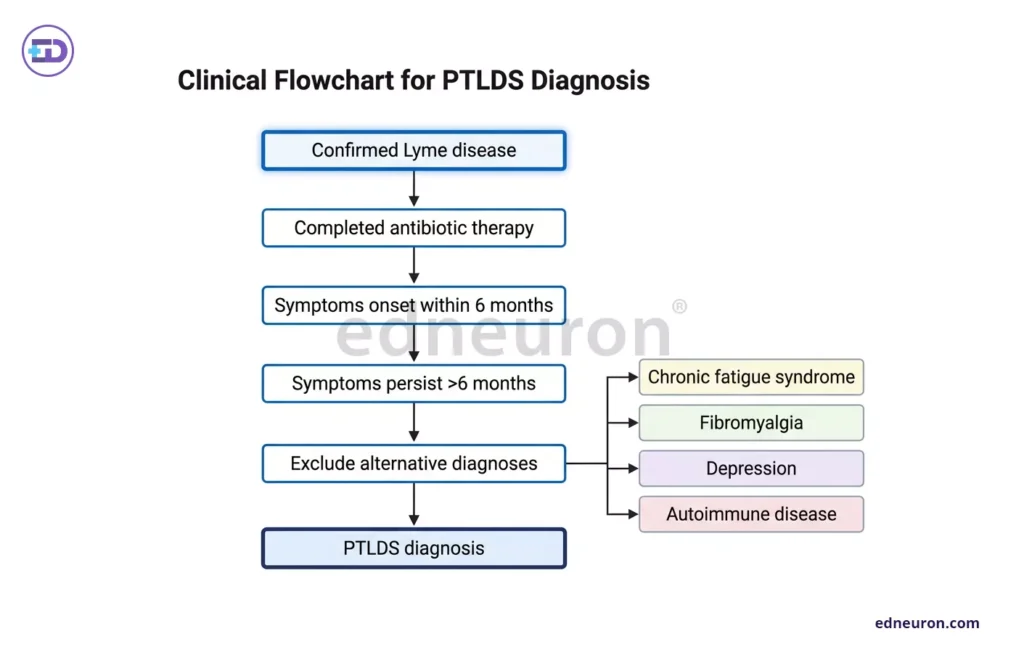
Fig 1: Evaluation strategy.
The Competing Pathophysiological Models
- Persistent Infection
The infection-persistence hypothesis draws its strongest support from xenodiagnostic models. Studies in non-human primates and murine systems have demonstrated the extraction of viable Borrelia in tissue reservoirs up to 3 months (joint capsule, collagen-rich structures, central nervous system) following antibiotic courses that cleared spirochetemia. These organisms that persisted under antibiotic pressure lacked genes on plasmids 1p25 and 1p28-1 (genes involved in invectivity) and were not cultivable. Such studies suggest that the persistence of these organisms after antibiotic therapy may be attributable to PTLDS. - Evading immune patrol
It has been postulated that immune evasion mechanisms involving tick saliva molecules and downregulation of outer membrane proteins (OspA/C) provide a biologically plausible scaffolding for spirochetal survival below treatment thresholds. The translational validity of this evidence, however, is poor. Reproducible detection of persistent viable organisms in human PTLDS has not been established, perhaps because of transient bacteremia and the absence of pathogens in human skin, unlike in mouse models. Xenodiagnostic studies and molecular methods have yielded conflicting results. The inference that animal persistence remains speculative and is insufficient to justify clinical decisions predicated on active infection. Moreover, therapy models based on the persistence of organisms offer no benefit to patients who are often prescribed long-term antibiotics. Moreover, deleterious effects are often associated with reduced immunity and dysbiosis of the gut flora. - Immune Dysregulation
Post-infectious immune sequelae suggest that the immune system is not in equilibrium after infection. Cytokine profiling in PTLDS cohorts has revealed elevations in pro-inflammatory mediators, including CCL19 and CXCL13, alongside signatures consistent with ongoing immune activation, which are associated with a 12-fold higher risk of PTLDS within 6-12 months. Anti-neural antibodies have been identified in subsets of patients, raising the possibility of either the release of autoantigen during active neural damage or the post-mitotic effect of Borrelia antigens on polyclonal B cells. This model aligns conceptually with other post-infectious syndromes with mechanistic links to molecular mimicry and cross-antigen reactivity such as rheumatic fever and post-streptococcal arthritis, in which the pathogen recedes, but the immune response does not. This suffers bitterly from its own evidential limitations because no biomarker reliably distinguishes PTLDS from recovered Lyme disease, active infection, or other immune-mediated fatigue states. C-C motifs Cytokine signatures are inconsistent across cohorts, likely reflecting patient heterogeneity. Neuroimaging identifies white matter changes in patients with PTLDS, suggesting altered immune-neural signaling. But whether these changes are causative, consequential, or correlative cannot be conclusively drawn. - PTLDS by virtue of neurobiological mechanisms also exhibit overlaps within the broader category of central sensitization disorders: fibromyalgia, myalgic encephalomyelitis/chronic fatigue syndrome, and post-viral syndromes. The initial infection and early vagal involvement trigger maladaptive plasticity in pain-processing pathways, autonomic regulation, and glial signaling, as well as cranial nerve palsies that persist even after the pathogen is eliminated. The symptomatic triad of PTLDS (fatigue, pain, cognitive dysfunction) maps closely onto this construct. The limitation of this model is its overlap with functional somatic disorders, which risks prematurely closing the diagnosis of a potentially neuroimmunological process. Central sensitization and peripheral immune dysregulation are not mutually exclusive, emerging evidence suggests bidirectional signaling between the immune system and the central nervous system that may perpetuate both. Intuition should not treat these hypotheses as mutually exclusive but rather as a Venn diagram or a layered model. Heterogeneity in PTLDS can then be thought of as an orchestra with initial infection triggering immune activation; in a subset of patients, immunological resolution is incomplete or dysregulated with persistent immune signaling altering central pain and fatigue pathways; and a self-perpetuating neuro-immune loop that sustains symptoms even in the absence of ongoing spirochetemia.
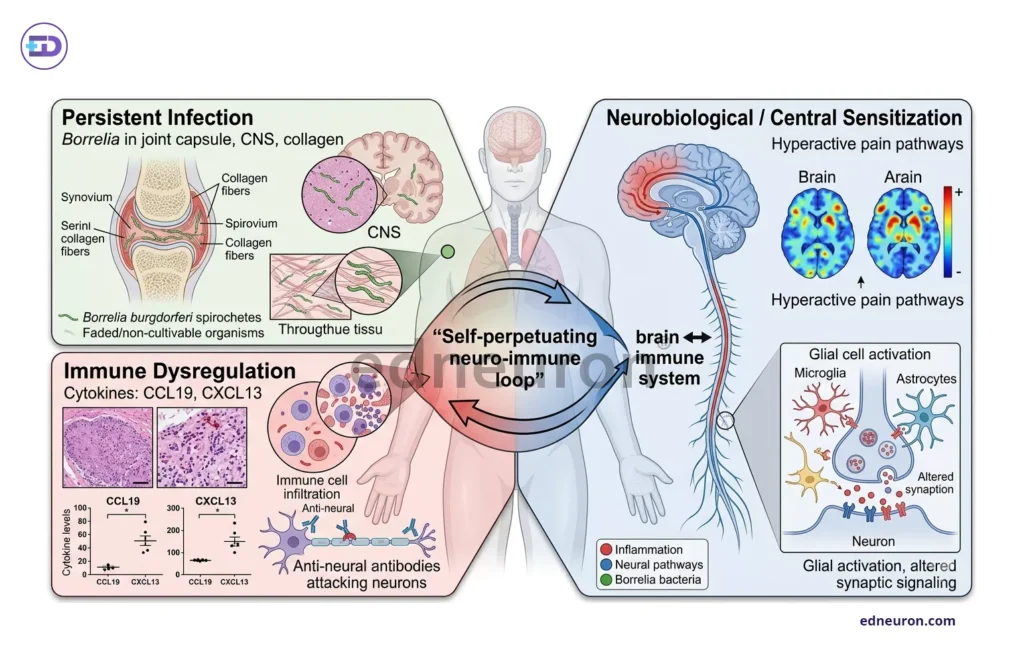
Fig 2: Comparative panel of various mechanisms causing PTLDS. Note persistent peptidoglycan causes chronic synovitis with a peculiar persistence in collagenous-rich sites.
Therapeutic Controversy
One pivotal NEJM trial – Klempner et al. (2001) enrolled well-characterized PTLDS patients and demonstrated no clinically meaningful benefit of prolonged intravenous or oral antibiotic therapy over placebo. Adverse events, including line infections and Clostridioides difficile colitis, were non-trivial. IDSA guidelines actively advise against extended antibiotic courses for persistent nonspecific symptoms once the patient has completed therapy. The advocacy for antibiotic retreatment in PTLDS reflects, in part, the absence of effective alternatives as immunomodulatory strategies, targeting cytokine signaling or anti-neural antibodies remain largely investigational. Multimodal approaches such as cognitive-behavioral therapy (CBT), kundalini yoga (Murray et al.), neuropathic agents (duloxetine, pregabalin), graded rehabilitation for deconditioning, and sleep restoration offer the best current evidence base. However, none have been validated in large PTLDS-specific trials. The fundamental problem is that we don’t fully understand the pathophysiology of the symptoms, and administering antibiotics to patients whose symptoms arise from central sensitization, or cognitive-behavioral therapy to those with active neuroinflammation, represents a mismatch that the absence of biomarkers makes unavoidable.
Conclusion
PTLDS endures as such an enigma not because we lack proof of its existence, but because current theories explain the mystery only partially, without integrating the whole truth. It is this perplexing mosaic of the current models that attempts to explain the full complexity of host-pathogen interaction. The infection may resolve while the immune system rages on; immune activation may subside even as the neural consequences echo. Moving beyond this requires cross-disciplinary trial design, patient phenotyping with reliable biomarkers, and commitment to a layered model in which infection, immunity, and neurobiology are understood as a dynamic, interacting ecosystem. Until then, clinical practice must proceed with as much humility as it requires caution.
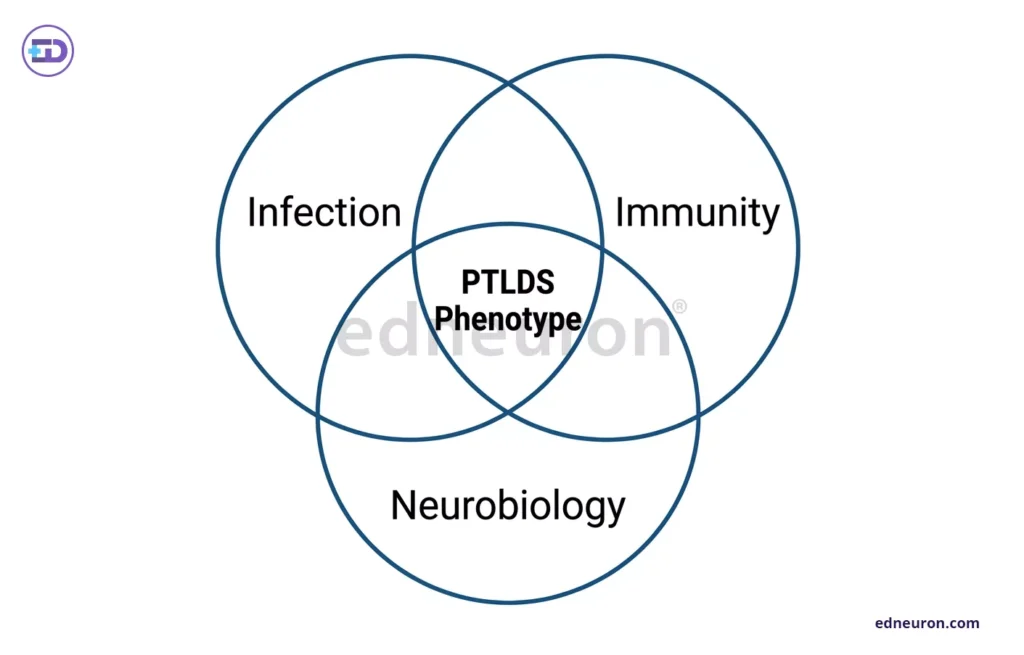
Fig 3: The PTLDS phenotype is characterized by a dynamic, altered interaction among immunity, host response, and neurobiology.
References
- Talbot NC, Spillers NJ, Luther P et al. Lyme Disease and Post-treatment Lyme Disease Syndrome: Current and Developing Treatment Options. Cureus. 2023 Aug 8;15(8):e43112. PMID: 37692614.
- Wester KE, Nwokeabia BC, Hassan R et al. Exploring the Mechanisms of Post-treatment Lyme Disease Syndrome. Cureus. 2024 Jul 20;16(7):e64987. PMID: 39161484.
- Bockenstedt LK, Gonzalez DG, Haberman AM, Belperron AA. Spirochete antigens persist near cartilage after murine Lyme borreliosis therapy. J Clin Invest. 2012 Jul;122(7):2652-60. Epub 2012 Jun. PMID: 22728937.
- Aucott JN, Soloski MJ, Rebman AW et al. CCL19 as a Chemokine Risk Factor for Posttreatment Lyme Disease Syndrome: a Prospective Clinical Cohort Study. Clin Vaccine Immunol. 2016 Sep 6;23(9):757-66. PMID: 27358211.
- Klempner MS, Hu LT, Evans J et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001 Jul 12;345(2):85-92. PMID: 11450676.
- Murray L, Alexander C, Bennett C et al. Kundalini Yoga for Post-Treatment Lyme Disease: A Preliminary Randomized Study. Healthcare (Basel). 2022 Jul 15;10(7):1314. PMID: 35885840.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi


