

Introduction
A wound that does not heal demands reconsideration. The patient presents with a decades-long history of lower extremity osteomyelitis, a persistently draining sinus tract managed with periodic wound care and episodic antibiotic therapy, and now, after years of the same antiquity, a new, friable mass is found at the wound margin. Deep tissue biopsy confirms squamous cell carcinoma (SCC). This case, which an orthopedician encounters with distressing frequency, even if the occurrence is quite rare but not unprecedented, is suffused with a common error: conflating chronicity with stability. A sinus tract that has drained for thirty years is considered a static scar. Unbeknownst to us, it is a biologically active tissue interface, perpetually negotiating between the crisis of repair and destruction, between inflammation and resolution, and, as accumulating evidence suggests, between regeneration and neoplastic transformation. The chronic wound, in the seat of evidenced familiarity, is most likely the wound that harbors a malignancy invisible to clinical expectation.
Beyond Persistent Infection
Chronic osteomyelitis has traditionally been understood as a relapsing infectious disease-a battle between host immunity and bacterial persistence, new bone formation and destruction in intramedullary and periosteal surfaces, punctuated by debridement, antibiotic suppression, and surgical reconstruction. This, while clinically operational, is biologically incomplete because it fails to capture the tissue-level consequences of that unresolved conflict. A chronically dysregulated wound-healing environment with a mean latency time between 20 and 50 years after onset of osteomyelitis that shares fundamental molecular architecture with other established pre-oncogenic niches. The chronic draining sinus tract represents more than just an anatomical conduit for purulent drainage that lessens the systemic toxicity. Over time, the wound undergoes cicatrization, epithelializing across the wound margins as squamous cells migrate and encroach on the lining of the fistula tract. The environment undergoes harsh inflammatory disruption and mechanical breakdown, with microbial colonization forming biofilms. This increases the likelihood of spontaneous mutations (in TP53 and other tumor suppressor genes). Such is the ecological niche that tussles between seasons of reactive hyperplasia and dysplastic transformation. One can draw parallels across the literature: Barrett’s esophagus arises in the context of chronic acid exposure and regenerative stress; Cholangiocarcinoma arises from chronically inflamed biliary epithelium, especially when compounded by parasitic infections such as Opisthorchis viverrini and Clonorchis sinensis. Marjolin’s ulcer, the prototypic malignancy of chronic wounds described by French physician Jean Nicolas Marjolin, develops at the margins of burn scars and pressure injuries subjected to prolonged inflammatory cycling. The chronic osteomyelitis fistula operates on the same principle, i.e., a persistent inflammatory repair ecosystem caught between the drudgery of healing and malignant evolution.
Mechanistic Architecture of Pre-Oncogenic Niche
The carcinogenic potential of the chronic sinus tract is not solitary molecular event but rather several reinforcing biological processes.
- Chronic cytokine exposure and NF-κB activation.
Persistent infection drives the ephemeral elaboration of pro-inflammatory mediators like TNF-α, IL-1β, and IL-6, which activate the NF-κB pathway, contributing to the nexus of inflammation-driven carcinogenesis. Cellular proliferation and TH-2 macrophage activation, inhibition of cellular apoptosis, and angiogenesis (VEGF), collectively propel cells towards the precipice of neoplastic transformation. The inflammatory cytokines also result in differentiation of macrophages into protumorigenic, profibrotic counterparts, oxidative stress, and genomic instability. Activated neutrophils and macrophages recruited to the chronic wound generate reactive oxygen species (ROS) as part of their antimicrobial response. Additionally, when bacterial clearance is evaded by immune patrol, the oxidative burden is still sustained, inflicting DNA damage, oxidizing guanine residues, and inducing strand breaks that activate impaired mismatch repair, further promoting de novo passenger mutations in these epithelial cells. - Biofilm persistence
Modern understanding of chronic osteomyelitis has shifted from a relapsing abscess model to a more host-pathogen interaction framework. Biofilm is the key concept driving the long-term persistence of organisms such as Staphylococcus aureus by virtue of their ability to produce adhesins, immunomodulatory proteins, and superantigens. Bacterial biofilms resist antibiotic penetration and evade phagocytic clearance through altered metabolic states, exopolysaccharide matrix production, and the release of leukocidin A/B (LukAB) and PVL, which directly kill neutrophils, macrophages, and other antigen-presenting cells by damaging cellular membranes and by directly suppressing IL-1β- and IL-12-dependent immunity. The result is macrophage polarization toward an M2-like, pro-fibrotic, and immunosuppressive phenotype-a microenvironmental configuration that mirrors the tumor-associated macrophage biology observed in established cancers. - Tissue hypoxia and HIF-1α signaling
Unrelenting cycles of inflammation within and around the osteomyelitic foci cause fibrous encapsulation, shunting off vascular supply to the sequestra, and edematous soft tissue creates zones of sustained tissue hypoxia, allowing translation of Hypoxia-inducible factor-1α (HIF-1α). Under oxygen stress, HIF-1α gets stabilized and promotes angiogenesis, metabolic reprogramming, and, critically, transcriptional programs associated with epithelial-to-mesenchymal transition (EMT). EMT-like plasticity in chronically stressed epithelium may represent a key permissive step toward invasive squamous carcinogenesis. - Fibro-inflammatory remodeling and stromal complicity
All the while, the wound now undergoes sculpting in ways that render the desmoplastic microenvironment indistinguishable from the cancer-associated stroma of established solid tumors. Chronic osteomyelitic stroma gets progressively rich in myofibroblasts, aberrant extracellular matrix, and pro-growth paracrine signals that actively support cellular survival and proliferation.
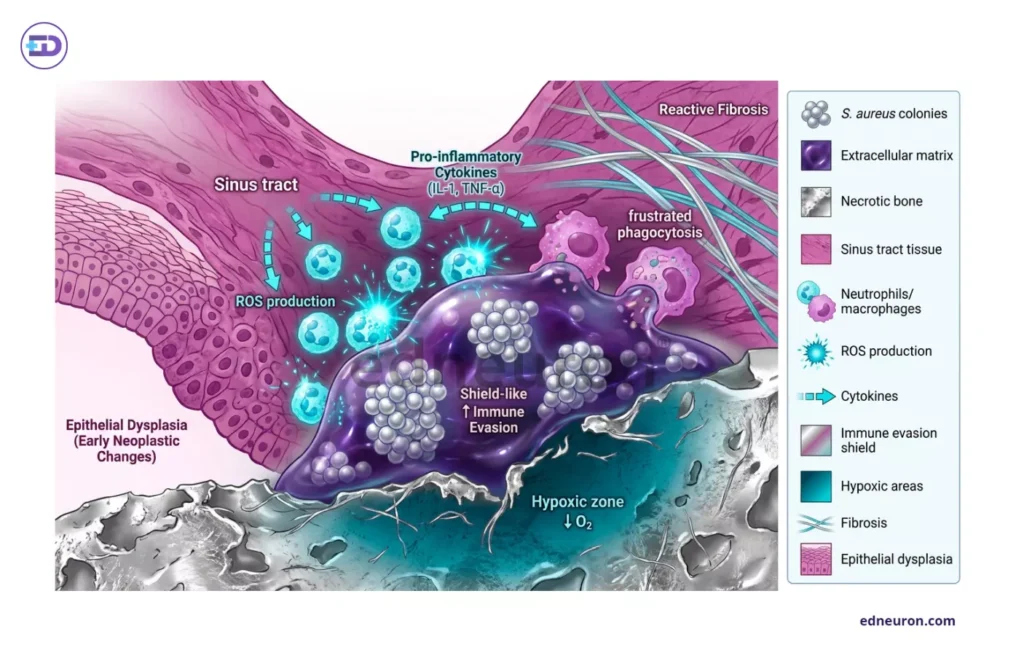
Fig 1: Magnified version of all factors in action to supplement the transition and compound damage.
Although multiple studies have established the biological plausibility of a correlation between the two, direct prospective evidence for causality between chronic osteomyelitis and squamous cell carcinoma remains incomplete. The mechanistic framework presented here is inferentially grounded in wound biology, inflammation science, and translational oncology, rather than proven by prospective cohort data.
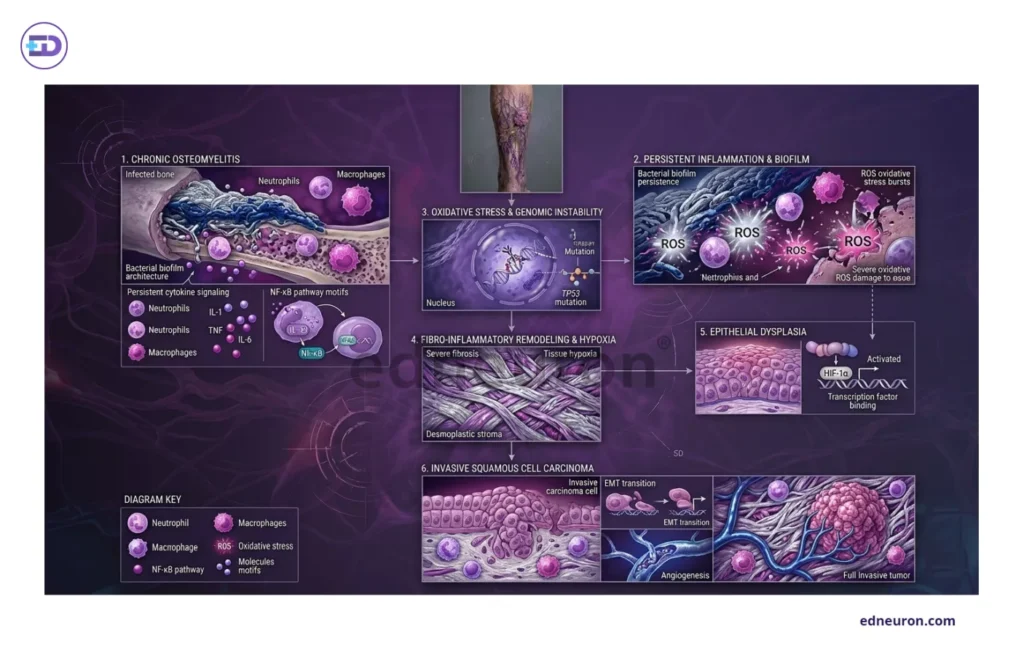
Fig 2: Translation of Chronic OM to SCC employs multidimensional interaction among inflammatory signals, ROS stress and EMT transition.
Histopathological Complexity and Diagnostic Traps
The diagnosis of malignant transformation within a chronic sinus tract is confounded at every level—clinical, radiological, and pathological.
Clinically
The presentation is deceptive because drainage is expected, pain is supposedly baseline, and radiological findings of cortical destruction and periosteal reaction overlap substantially between progressive osteomyelitis and bone-invasive carcinoma; for example, MR images amplify the problem, with the same signals showing marked periosteal enhancement.
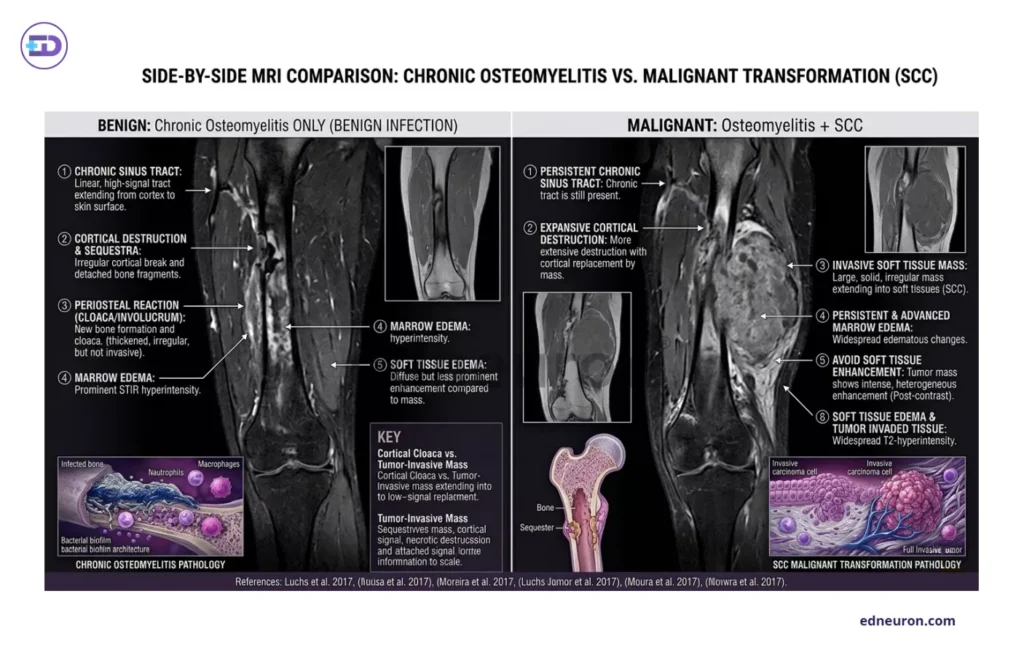
Fig 3: Side-by-side MRI comparison: Chronic osteomyelitis vs Malignant SCC.
Pathologically
The distinction between reactive and malignant epithelial proliferation is among the most challenging in surgical pathology. Pseudoepitheliomatous hyperplasia (PEH), almost a doppelganger, is a reactive, non-neoplastic, exuberant epithelial proliferation that occurs in chronically inflamed wounds and can closely mimic well-differentiated SCC in its architecture and cytology. To top it off, inflammation-induced reactive atypia, nuclear pleomorphism, and regenerative mitotic activity further obscure the distinction.
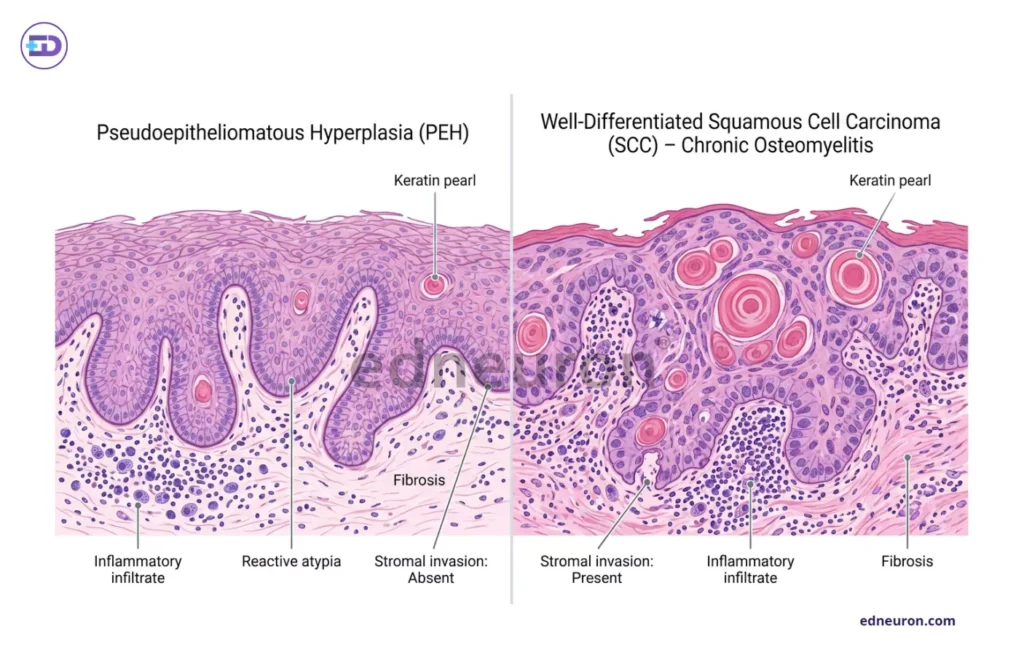
Fig 4: Side-by-side comparative panel of PEH and SCC.
Diagnostic methodologies like superficial biopsy sampling, which captures only the most reactive layers of the wound surface, are insufficient, yielding inconclusive results and missing the deeper invasive component of an evolving carcinoma. Perhaps the extraordinary latency (20-50 years) is not evidence of a rare transformation but rather suggests that surveillance is still lagging and that the disease is recognized only after the window for optimal management has closed.
Clinical Vigilance and Conclusion
Any of the following changes in a previously stable chronic sinus tract warrant urgent reassessment:
- Enlarging soft-tissue mass beyond the expected wound margins or a firm, infiltrative quality on palpation.
- Change in pain character or intensity. A shift from chronic, stable pain to progressive or nocturnal pain may reflect periosteal or neural involvement by tumor.
- Bleeding from the sinus tract. Spontaneous or contact bleeding from granulation tissue should never be attributed to reactive change without histological confirmation.
- Alteration in drainage character or odor, particularly increased volume, altered viscosity, or a qualitative change in malodor not explained by intercurrent infection.
- Failure to respond to directed antimicrobial therapy. Progressive wound deterioration despite adequate antibiotic and surgical management.
- Excessive or exuberant granulation tissue, particularly with surface friability or verrucous morphology.
- Regional lymphadenopathy: inguinal or popliteal adenopathy in the setting of lower-extremity osteomyelitis should prompt immediate oncological evaluation.
The takeaway point is that chronic sinus tracts should never be treated as static entities that require only passive wound management.
- Longitudinal photography
- Periodic deep-tissue biopsy at defined intervals
- Low-threshold cross-sectional imaging embodies a minimum standard of care for patients.
- Some authors have proposed intentional maintenance of chronic sinus tracts as a palliative strategy in selected patients with refractory disease. Such a strategy, if adopted, must incorporate structured oncological surveillance.
Evaluative decision-making in the case of long-standing osteomyelitis must operate at a crossroads, mediating conversations among the surgeon, the immunologist, the pathologist, and the oncologist. We do not yet possess the prospective data necessary to define optimal surveillance intervals, biopsy thresholds, or imaging protocols for this population. This in itself is an argument for urgency. What we can probably offer at the table is the institutional commitment to treat the chronic wound as an entity deserving of longitudinal oncological vigilance.
References
- Moura DL, Ferreira R, Garruço A. Malignant transformation in chronic osteomyelitis. Rev Bras Ortop. 2017 Mar 8;52(2):141-147. PMID: 28409129.
- Pundkare GT, Tawde A, A K, Mirchandani N, Lodha S. Squamous Cell Carcinoma Arising in Chronic Osteomyelitis: A Rare Presentation. Cureus. 2023 Dec 1;15(12):e49783. PMID: 38164310.
- Bazaliński D, Przybek-Mita J, Barańska B, Więch P. Marjolin’s ulcer in chronic wounds – review of available literature. Contemp Oncol (Pozn). 2017;21(3):197-202. PMID: 29180925.
- Greten FR, Grivennikov SI. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity. 2019 Jul 16;51(1):27-41. PMID: 31315034.
- Rybinski B, Franco-Barraza J, Cukierman E. The wound healing, chronic fibrosis, and cancer progression triad. Physiol Genomics. 2014 Apr 1;46(7):223-44. PMID: 24520152; PMCID: PMC4035661.
- Masters EA, Ricciardi BF, Bentley KLM, Moriarty TF, Schwarz EM, Muthukrishnan G. Skeletal infections: microbial pathogenesis, immunity and clinical management. Nat Rev Microbiol. 2022 Jul;20(7):385-400. PMID: 35169289; PMCID: PMC8852989.
- Luchs JS, Hines J, Katz DS, Athanasian EA. MR imaging of squamous cell carcinoma complicating chronic osteomyelitis of the femur. AJR Am J Roentgenol. 2002 Feb;178(2):512-3. PMID: 11804933.
- Sankaran-Kutty M, Corea JR, Ali MS, Kutty MK. Squamous cell carcinoma in chronic osteomyelitis. Report of a case and review of the literature. Clin Orthop Relat Res. 1985 Sep;(198):264-7. PMID: 4028559.
- Luchs JS, Hines J, Katz DS, Athanasian EA. MR imaging of squamous cell carcinoma complicating chronic osteomyelitis of the femur. AJR Am J Roentgenol. 2002 Feb;178(2):512-3. PMID: 11804933.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



