

Introduction
The idea of cancer of unknown primary (CUP) being the orphan cancer that could be traced back to no parental primary tissue origin, even after aggressive investigations, although it is clinically expedient, may fundamentally mischaracterize the biology of a substantial subset of cases. It’s been hypothesized that this entity might not just have one signature of genetic profile that could pinpoint a parent tissue organ, but rather a secondary genetic identity independent of primary site, pro-metastatic, one in which systemic metastatic competence emerges before local tumor dominance is established. Scrutiny under the analytical lens of parallel progression theory, chromosomal instability, the limitations of tissue-of-origin molecular classifiers, and therapy targeting the home genetic markers, and the hypothesis of primary tumor regression or immunologic dormancy, it is indeed rendered plausible to consider that the dissemination in CUP may constitute an opening act rather than a terminal event. We acknowledge the heterogeneity inherent in this including the meaningful survival benefit observed in molecularly guided therapy subsets (increased response to combination platinum chemotherapy in patients with showe strong co-expression of p53 and Bcl-2, Briasoulis E et al.) while maintaining that lineage assignment alone cannot fully capture the biological distinctiveness of unfavorable CUP (no benefit conferred in patients with non-expression of HER-2 and no difference in overall survival between patients overexpressing and not expressing HER-2, Hainsworth JD et al.). If CUP does, in fact, represent an independent evolutionary trajectory, its treatment must address the biology of metastasis, not the assumed biology of an origin it may never have consolidated.
Oncology is organized around the assumption of origin, the lighthouse to guide therapy and prognosis. The discipline’s taxonomy, its treatment algorithms, its clinical trials, and its biomarker frameworks all presuppose that cancer announces itself first at a primary anatomical site, expands locally, and then disseminates. Cancer of unknown primary (CUP) perturbs this very foundation. Here is a malignancy that presents systemically, often with multiple metastatic deposits in 3 or more organs, yet produces no identifiable primary tumor despite exhaustive imaging, endoscopy, serology, and molecular profiling. In more than 80% of antemortem case series and 30-70% post mortem autopsies, the primary tumor remains unidentified. The reflexive interpretation often arises from diagnostic intuition: the primary tumor was too small to be clinically detected, too regressed or undifferentiated to be characterized. While this explanation is undoubtedly correct for some patients, it is increasingly insufficient as a universal account. The clinical behavior of unfavorable CUP: its unusual metastatic distributions, its refractoriness to lineage-based therapy, and its median survival (3–6 months in unfavorable and 10–16 months in favorable subsets) despite modern platinum regimens suggests that something more fundamental may be at work. The possibility that a subset of CUP cases represents a biologically distinct metastatic phenotype warrants rigorous mechanistic investigation.
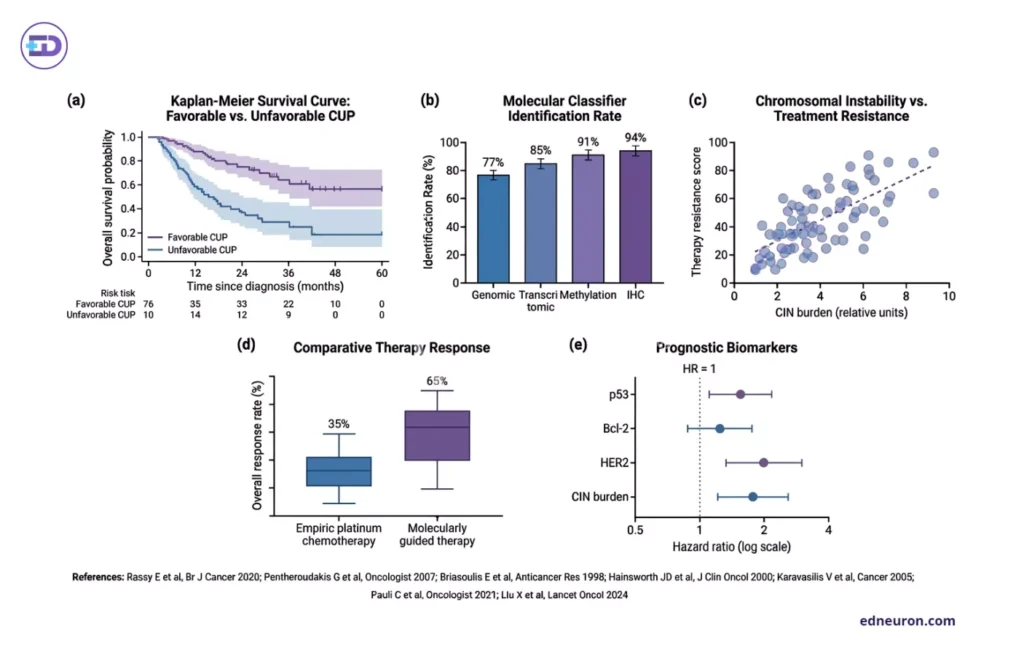
Fig 1 : Multimodal prognostic and molecular stratification framework in carcinoma of unknown primary (CUP).
Why CUP May Be Biologically Distinct
The argument for biological distinctiveness rests on several observations that resist the occult-primary explanation. CUP consistently violates the canonical rules of organotropism-the Paget seed-and-soil logic-as CUP metastases appear in atypical distributions, often in multiple organ systems simultaneously, without a coherent pattern traceable to a presumed origin. This suggests not a competent primary tumor whose metastases have simply outgrown it, but rather a tumor that achieved early epithelial-to-mesenchymal (EMT) transition. It then becomes more befitting as Rassy E and colleagues advanced the explicit reframing of CUP as ‘primary metastatic cancer’, a conceptual inversion in which the metastatic event is the primary biological fact, not a downstream consequence. This is not merely rhetorical; if dissemination is the founding event, then the therapeutic question is not ‘what organ did this tumor come from’ but ‘what evolutionary pressures produced a cell capable of systemic competence before local dominance.’ The two questions lead to different biologies, different targets, and different clinical trial designs.
Early Dissemination and the Metastatic Hypothesis
The parallel progression theory, derived from phylogenetic analyses of matched primary and metastatic tumor specimens, demonstrates that polyclonal metastatic seeding can occur when the primary tumor is still microscopic and before it has achieved the architectural organization and clonal dominance visible on imaging or pathology. Crucially, the metastatic clone is often genetically divergent from the primary at the time of dissemination, exhibiting increased expression of MMP-2, MMP-9, and VEGF, suggesting enrichment in such protein transcripts plays an important role in stromal proteolysis, invasive migration, and angiogenesis. Interestingly, Karavasilis V et al. found tissue inhibitors of these metalloproteinases, specifically TIMPs, to be associated with poor outcomes in CUP subsets, reconciling existing empirical evidence that TIMPs may have a multifaceted role in cancer metastasis, with cells acquiring competence through independent evolutionary pressure rather than sequential primary-to-metastatic progression. Immunologic editing where the progressive selection of tumor variants that evade immune surveillance may, in principle, act with differential intensity at different tumor sites. A primary tumor embedded in immunologically active tissue may be eliminated, while its disseminated descendants, seeded into more permissive microenvironments, escape and expand. Immune checkpoint biology has demonstrated that tumor regression is not exceptional but achievable when immune cells are adequately sensitized to the cancer cell fingerprint (epitope). Whether, under this immune pressure, primary foci are selectively sterilized while metastatic ones are spared is a mechanistic question that CUP uniquely positions to answer.
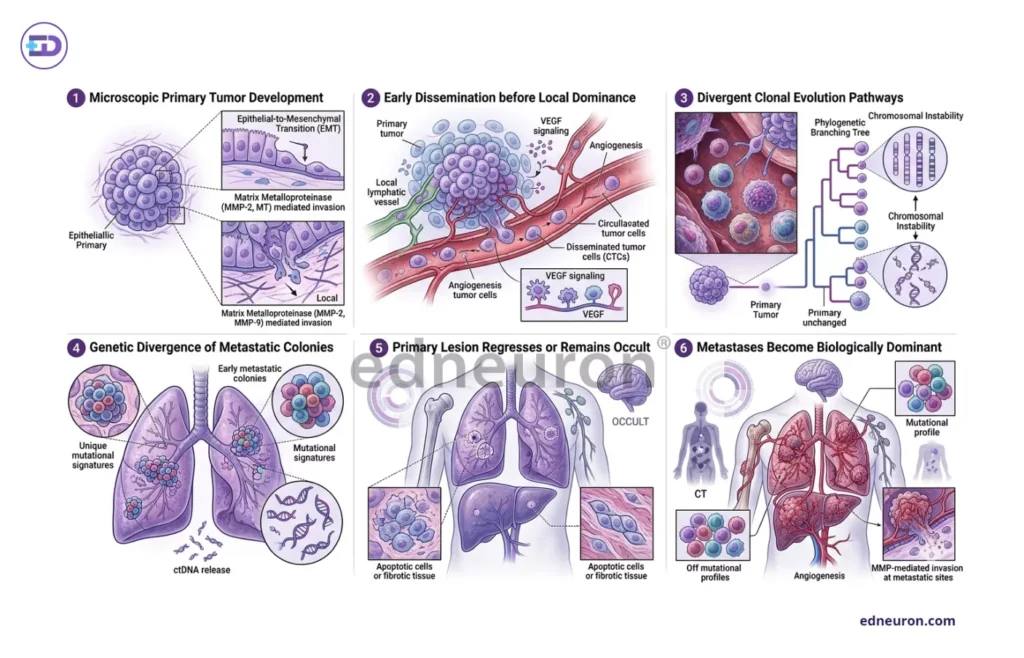
Fig 2 : Various hallmark features of CUP.
Chromosomal Instability and the Refractoriness Phenotype
Among the molecular features of unfavorable CUP, chromosomal instability (CIN) is central. CIN encompassing aneuploidy, copy-number instability, and the ongoing generation of genomically diverse clonal subpopulations is not merely a marker of aggressive disease. Such aberrations and aneuploidy (70-90% cup tumors) become the engine of plasticity and mouldability, enabling rapid clonal adaptation to therapeutic selective pressure and microenvironmental variation. The genomic profiling studies nested within the CUPISCO framework have documented high copy-number burden and broad mutational chaos in unfavorable CUP. If CIN is operating at this intensity, it may explain both the unusual metastatic distributions because phenotypic plasticity dissolves organotropic constraints and the poor response to lineage-based therapy, because the tumor is not behaving according to the rules of its lineage of origin. Resistance, in this framework, is not incidental. It is a predicted consequence of a biology that has already departed from canonical tissue behavior.
The failure of the conventional lineage-based approach in CUP
The advent of gene expression profiling and multi-analyte molecular classifiers offered, at least conceptually, a path through the CUP problem. If the tumor’s transcriptional lineage could be identified despite the absence of a visible primary, site-specific therapy could be applied. Lineage genetic signatures reflect developmental origin—-> developmental origin shapes receptor expression—-> pathway dependency, and drug sensitivity. Advanced diagnostic machinery, such as PET scans having 87% sensitivity and 71% specificity, along with holistic molecular profiling, including microRNA assays and quantitative PCR low-density arrays, has yielded identification rates of 77–94%. However, the translation of such technological promises into clinical meaning has remained inconsistent, with no proven survival benefit in either empirically or molecularly guided therapies. A classifier assigns a cell’s developmental ancestry; it cannot assign its immunological edits’ trajectory, and identifying a tumor’s origin does not necessarily allow its evolutionary visualization. The Fudan CUP-001 trial demonstrating a progression-free survival advantage for 90-gene expression assay-guided site-specific therapy over empiric chemotherapy [95% CI 8·4-11·9] vs 6·6 months [5·5-7·9]; unadjusted hazard ratio 0·68 [95% CI 0·49-0·93]; p=0·017) defies any monolithic claim that origin is irrelevant still median survival remained measured in months. Predicting the antiquity of the primary tumor helps guide treatment selection for some patients. Still, it does not and cannot address the reality of metastasis, which has long departed from lineage-defined behavior; the biology of metastasis eclipses that of origin.
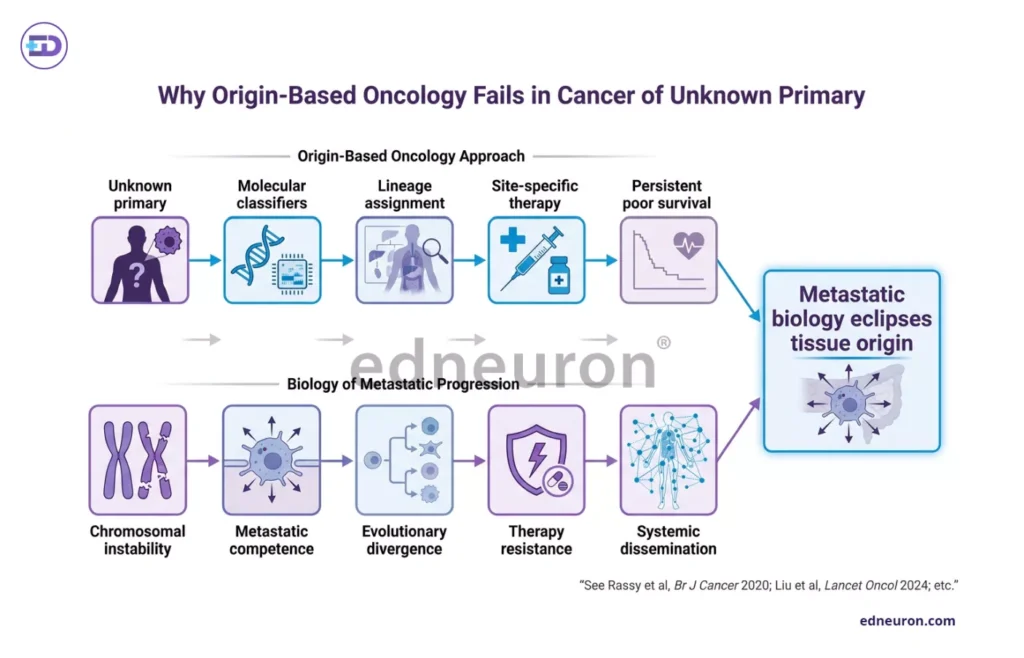
Fig 2 : Diagrammatic representation of why conventional origin-based chemotherapy fails in CUP.
Conclusion
- Going beyond the prediction of the primary site to find therapeutic vulnerabilities by adopting molecular profiling in CUP to capture metastatic profile by investigating CIN burden, heterogeneity indices, immune microenvironment, and pathway activation mechanism.
- Asking the right question: rather than ‘what does this tumor resemble,’ the question should be ‘what is this tumor doing, and what vulnerabilities has its evolutionary trajectory created?’ Immunotherapy, which acts on the metastatic microenvironment rather than on lineage-specific pathways, may be particularly relevant in CUP subsets characterized by high mutational burden and CIN-associated neoantigen generation.
If metastasis can precede local tumor consolidation, then the assumption that malignancy must stem from a locally dominant tumor is an historical artifact of a phenotype-first nosology rather than a law. CUP forces us to confront the possibility that, in some circumstances, the capacity for dissemination is not cancer’s final destiny or ultimate goal. It may be its first occupation. ‘Primary metastatic cancer’ with defined molecular and evolutionary substrates is not just a rename. It douses us with an accurate understanding of how malignancy sometimes evolves.
References
- Rassy E, Assi T, Pavlidis N. Exploring the biological hallmarks of cancer of unknown primary: where do we stand today? Br J Cancer. 2020 Apr;122(8):1124-1132. PMID: 32042068.
- Pentheroudakis G, Briasoulis E, Pavlidis N. Cancer of unknown primary site: missing primary or missing biology? Oncologist. 2007 Apr;12(4):418-25. PMID: 17470684.
- Briasoulis E, Tsokos M, Fountzilas G, et al. Bcl2 and p53 protein expression in metastatic carcinoma of unknown primary origin: biological and clinical implications. A Hellenic Co-operative Oncology Group study. Anticancer Res. 1998 May-Jun;18(3B):1907-14. PMID: 9677443.
- Hainsworth JD, Lennington WJ, Greco FA. Overexpression of Her-2 in patients with poorly differentiated carcinoma or poorly differentiated adenocarcinoma of unknown primary site. J Clin Oncol. 2000 Feb;18(3):632-5. PMID: 10653878.
- Karavasilis V, Malamou-Mitsi V, Briasoulis E et al. Matrix metalloproteinases in carcinoma of unknown primary. Cancer. 2005 Nov 15;104(10):2282-7. PMID: 16220559.
- Pauli C, Bochtler T, Mileshkin L et al. A Challenging Task: Identifying Patients with Cancer of Unknown Primary (CUP) According to ESMO Guidelines: The CUPISCO Trial Experience. Oncologist. 2021 May;26(5):e769-e779. PMID: 33687747.
- Liu X, Zhang X, Jiang S et al. Site-specific therapy guided by a 90-gene expression assay versus empirical chemotherapy in patients with cancer of unknown primary (Fudan CUP-001): a randomized controlled trial. Lancet Oncol. 2024 Aug;25(8):1092-1102. PMID: 39068945.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



