

Introduction
In the landscape of neurodevelopmental disorders, the autonomic nervous system often occupies a treacherous middle ground between neurology and cardiology. We frequently rely on the “cardio-protective” reputation of beta-blockers like propranolol to dampen paroxysmal sympathetic hyperactivity; “autonomic storms”, that characterize conditions such as Rett Syndrome (RTT). The clinical assumption is straightforward: block the beta-adrenergic receptors, and you mitigate the somatic manifestations of anxiety, tachycardia, and diaphoresis. However, when the underlying neurobiology involves profound brainstem immaturity, our standard pharmacological shields can behave in unexpectedly paradoxical ways. This case challenges the universality of beta-blockade as a stabilizing force, revealing a fragile autonomic equilibrium in which the heart and brainstem are in a state of precarious, atypical feedback.
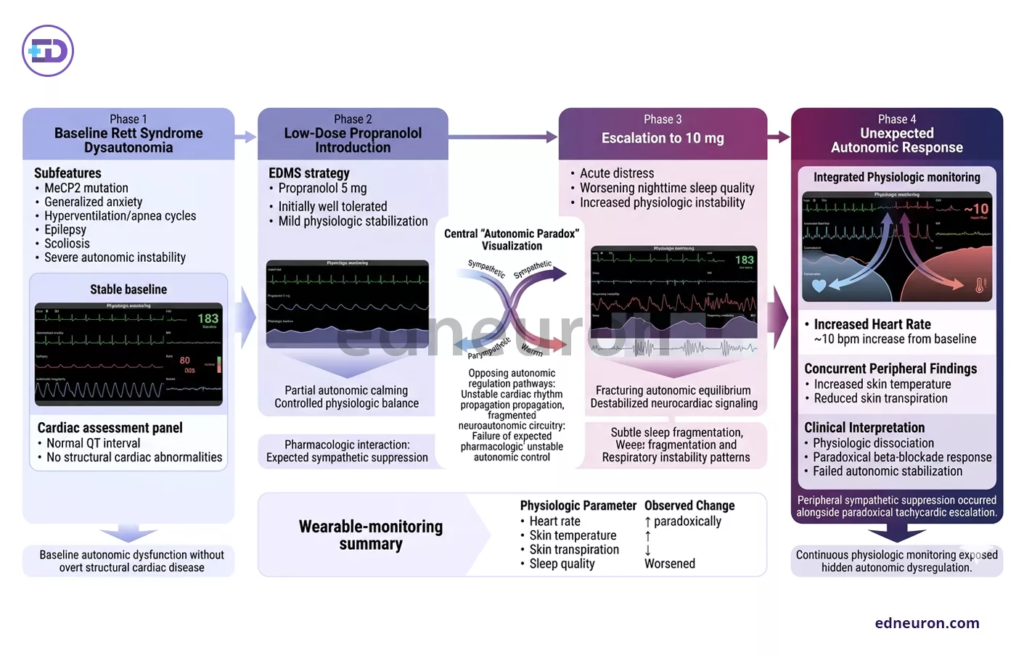
Fig 1 : Wearable physiologic monitoring revealed paradoxical tachycardic escalation despite peripheral sympathetic suppression following propranolol dose escalation in Rett syndrome.
Case Presentation
A 13-year-old girl with a confirmed genetic diagnosis of RTT (MeCP2 mutation) was referred for management of generalized anxiety and severe dysautonomia. Her clinical profile was a classic RTT constellation: disordered breathing (concomitant hyperventilation and apnea), epilepsy, and scoliosis. Critically, her baseline cardiac evaluation was unremarkable, showing no QT prolongation or structural abnormalities.
Using the “Effective Dosing with Minimum Side Effects” (EDMS) strategy, we introduced propranolol. Initially, 5 mg was well-tolerated, but an escalation to 10 mg triggered acute distress and a marked worsening of nighttime sleep quality. Continuous 24-hour physiological monitoring via wearable technology revealed an unexpected finding: a dose-dependent, paradoxical increase in average heart rate. At 10 mg, her heart rate increased by approximately 10 beats per minute from baseline, despite concurrent increases in skin temperature and decreases in skin transpiration. This physiological divergence forced an immediate termination of the treatment.
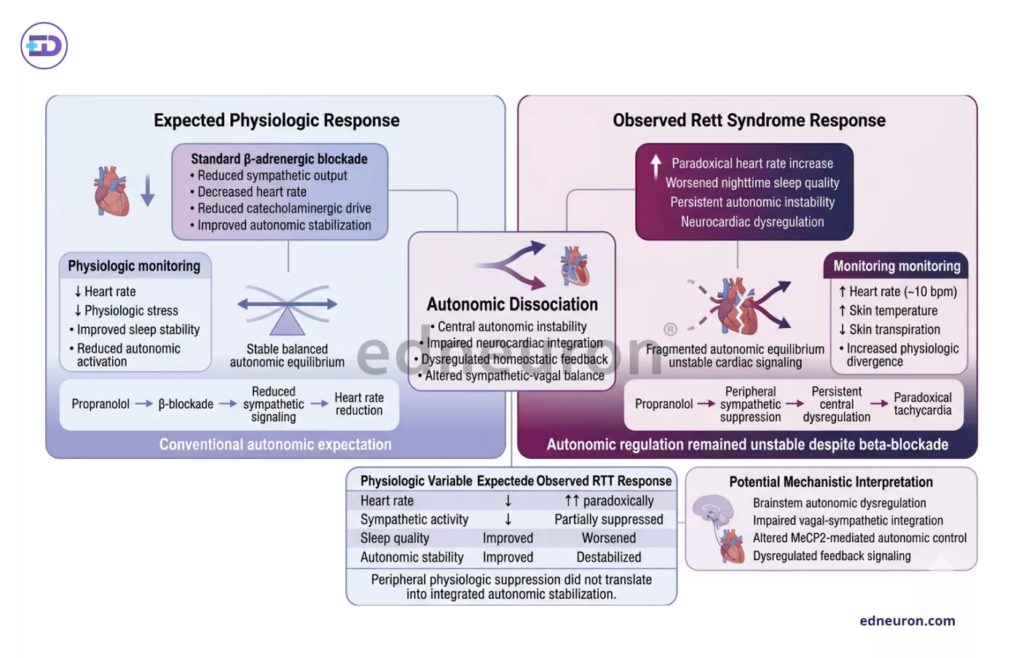
Fig 2 : In Rett syndrome, propranolol-induced peripheral sympathetic suppression may paradoxically coexist with worsening neurocardiac instability and increased heart rate.
Clinical Analysis / Discussion
What makes this case notable is the subversion of a fundamental tenet of pharmacology. Propranolol, by definition, is a sympatholytic agent and should not drive heart rate upward. To interpret this, we must look beyond the myocardium to the brainstem. RTT is a “synaptopathy” driven by loss of MeCP2 function, which disrupts the development of inhibitory and excitatory pathways in the brainstem.
The clinical uncertainty here arises from a unique autonomic architecture: RTT patients often exhibit uncontrolled, albeit normal sympathetic tone. This is not due to a surplus of “gas” (sympathetic drive) but a failure of the “brakes” (minimal negative feedback from the parasympathetic system). A plausible explanation for the tachycardia is that in the context of extreme brainstem immaturity, blocking peripheral beta-receptors may inadvertently disrupt a fragile compensatory mechanism or trigger a central sympathetic surge that the weak parasympathetic branch cannot abrogate.
This clinical observation mirrors troubling findings in murine models. Studies of MeCP2-deficient mice have shown that propranolol fails to prevent ventricular tachycardia or QTc prolongation. By integrating this literature with our patients’ data, we observe a consistent failure of beta-blockers to confer the expected cardioprotection in the RTT phenotype. The traditional mechanism, beta-adrenergic receptor blockade, appears insufficient to overcome the systemic sympathetic-parasympathetic imbalance inherent to the disorder.
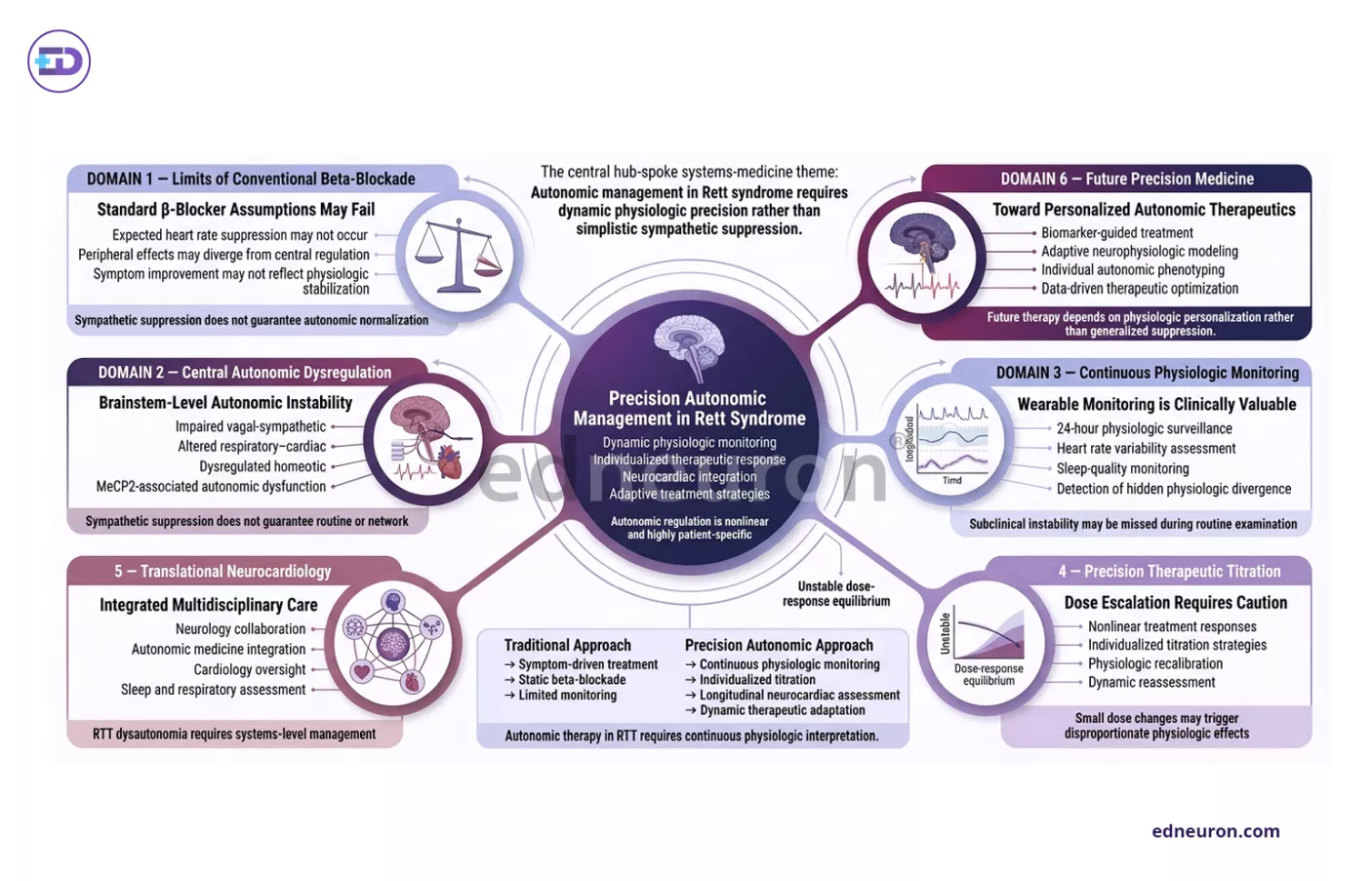
Fig 3: Paradoxical autonomic responses in Rett syndrome highlight the need for individualized physiologic monitoring and precision neurocardiac management beyond conventional beta-blockade paradigms.
Clinical Implications
This case serves as a stark reminder that in rare neurodevelopmental disorders, “standard” treatments require rigorous monitoring. The use of propranolol in RTT should be approached with extreme caution, as the paradoxical heart rate response may go undetected without continuous physiological tracking. Furthermore, it highlights the importance of psychophysiological profiling. If a clinician relies solely on the Efficacy Index or subjective reports of “distress,” they might miss the underlying autonomic instability driving that distress. The variability of RTT phenotypes—driven by X-linked inactivation—means that while some patients might tolerate beta-blockers, others may face a clinical worsening that masquerades as primary illness progression.
Conclusion
In Rett Syndrome, the heart is often the messenger for a deeper brainstem dysfunction. This case demonstrates that the “brakes” of the autonomic nervous system are not just diminished; they are fundamentally rewired. When treating synaptopathies, we must remain cognizant that the brainstem’s immaturity can turn a stabilizer into a disruptor, making the pursuit of “cardio-protection” a complex, and sometimes paradoxical, endeavor.
References
- Santosh PJ, Bell L, Lievesley K, Singh J, Fiori F. Paradoxical physiological responses to propranolol in a Rett syndrome patient: a case report. BMC Pediatr. 2016;16:194. doi:10.1186/s12887-016-0734-3. PMID: 27899087; PMCID: PMC5129599. Open-access case report discussing dysautonomia, sympathetic-parasympathetic imbalance, and paradoxical β-blocker response in Rett syndrome.
- Zhang P, Li Y, Nie K, Wang L, Zhang Y. Hypotension and bradycardia, a serious adverse effect of piribedil: a case report and literature review. BMC Neurol. 2018;18(1):221. doi:10.1186/s12883-018-1230-1. PMID: 30594184; PMCID: PMC6307137. Open-access pharmacovigilance-oriented case report focusing on dopamine agonist-induced autonomic cardiovascular dysfunction in Parkinson disease therapy.
- Leão P, Figueiredo P. Autonomic hyperreflexia after spinal cord injury managed successfully with intravenous lidocaine: a case report. Patient Saf Surg. 2016;10:10. doi:10.1186/s13037-016-0098-5. PMID: 26997874; PMCID: PMC4790546. Open-access case report highlighting pharmacologic suppression of autonomic dysreflexia during urological intervention in spinal cord injury.
- Cheshire WP, Goldstein DS. Autonomic uprising: the tilt table test in autonomic medicine. Clin Auton Res. 2019;29(2):215-230. doi:10.1007/s10286-019-00598-9. PMID: 30737544. Advanced review with multiple clinical autonomic case correlations and strong pharmacophysiologic discussion relevant to dysautonomia and cardiovascular autonomic testing.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India


