

Introduction
In the landscape of modern cardiac surgery, perioperative stroke remains a haunting complication that not only increases mortality but also fundamentally alters the trajectory of patient recovery. While surgical techniques have advanced, the incidence of stroke is frequently underestimated, as systematic neurological screening and postoperative magnetic resonance imaging often reveal far more cerebral damage than clinical observation suggests. The central clinical dilemma lies in the “hostile aorta”—a territory where the necessity of surgical access collides with the risk of dislodging atherosclerotic debris. What emerges is not a simple choice between techniques, but a complex risk-benefit calculus centered on minimizing aortic manipulation without compromising the primary procedural goals.
The Intimal Culprit: Mechanistic Distinctions
Clinically, we must distinguish between two distinct pathophysiological entities: intimal atherosclerosis and medial calcification. Intimal disease, often referred to as “soft plaque,” is the primary driver of embolic stroke, as most debris captured during surgery consists of fibrous atheroma tissue. Conversely, medial calcification—while presenting mechanical challenges for clamping and leading to potential aortic dissection—does not appear to increase the stroke rate as significantly once intimal disease is ruled out. This distinction is critical because the benefit of preventive strategies is entirely dependent on the specific severity and stage of the disease. Intraoperative screening with epiaortic ultrasound remains the gold standard for this assessment, as transesophageal echocardiography frequently fails to visualize the distal ascending aorta due to interference from the left main bronchus.

Fig 1: Intraoperative deployment of a stented embolic protection device within a plaque-burdened aorta to mitigate the risk of perioperative stroke during cardiac surgery.
The Manipulation Paradox in Revascularization
In coronary artery bypass grafting (CABG), surgical tension centers on the degree of clamping. For patients with severe intimal disease, the “no-touch” off-pump technique (OPCAB) offers a clear benefit in reducing stroke risk by avoiding aortic manipulation entirely. However, this strategy introduces a secondary tension: the technical requirement for experienced surgeons to ensure that avoiding the pump does not result in incomplete revascularization or inferior long-term outcomes. Evidence suggests that while partial clamping may be safe in mild disease, the additional wall shear stress and “sandblasting effect” from cannulas can dislodge vulnerable plaques in moderate to severe cases. What complicates this further is that while endovascular interventions like stenting are often seen as “conservative,” they do not necessarily decrease stroke risk compared to no-touch surgery and may be associated with lower survival in patients who have a clear surgical indication.
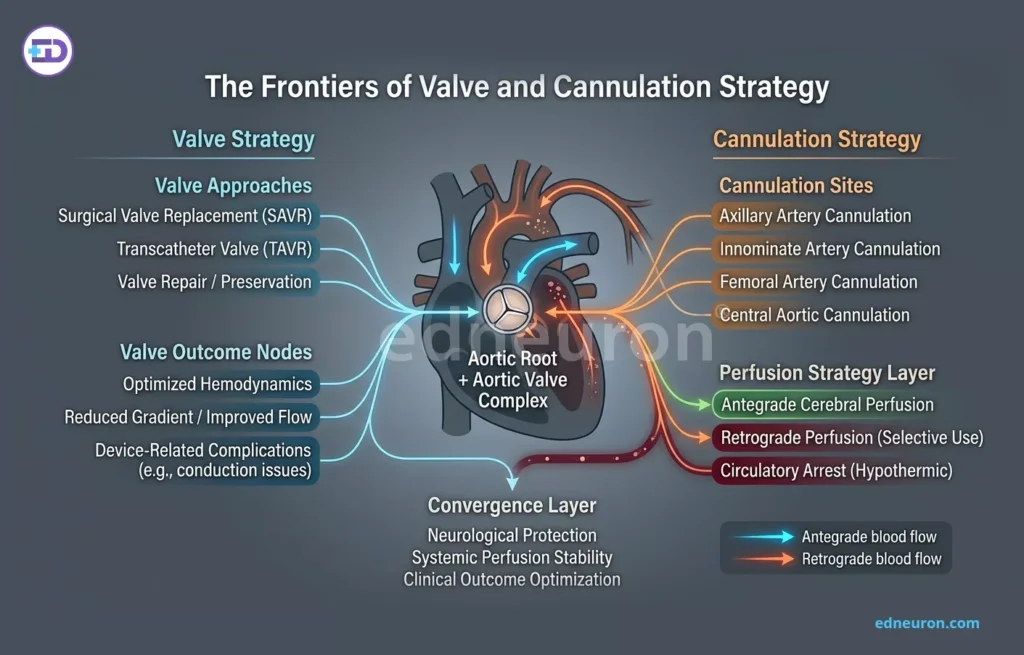
Fig 2: Cannulation approach to different segments of the heart, as well as intercoronary segments.
The Frontiers of Valve and Cannulation Strategy
Surgical aortic valve replacement (SAVR) presents a more rigid challenge, as cardiopulmonary bypass and aortotomy are imperative. While transcatheter aortic valve replacement (TAVR) is frequently used in patients with a “porcelain aorta,” its role in patients with predominantly intimal disease remains poorly defined, as the necessary wire manipulation may dislodge atherosclerotic debris. When traditional central cannulation is impossible, axillary artery cannulation has emerged as a superior alternative to femoral access. Retrograde perfusion from the femoral artery in the presence of a diseased descending aorta significantly increases embolization risk, whereas axillary access alters blood flow patterns in a manner that may decrease the delivery of microparticles to the cerebral circulation.
Clinical Outcomes and Real-World Implications
The translation of these strategies into practice reveals that a one-size-fits-all approach is insufficient. In high-risk populations, such as those with carotid disease—which affects approximately 50% of patients with systemic atherosclerosis—the stakes of aortic manipulation are even higher. For these complex patients, hybrid approaches or radical strategies like aortic replacement under deep hypothermic circulatory arrest may be considered, though they carry a high procedural burden and significant risks of postoperative bleeding or renal failure. The decision to recommend a specific approach must be patient-centered, weighing the severity of intimal thickening against the surgeon’s expertise in alternative techniques.
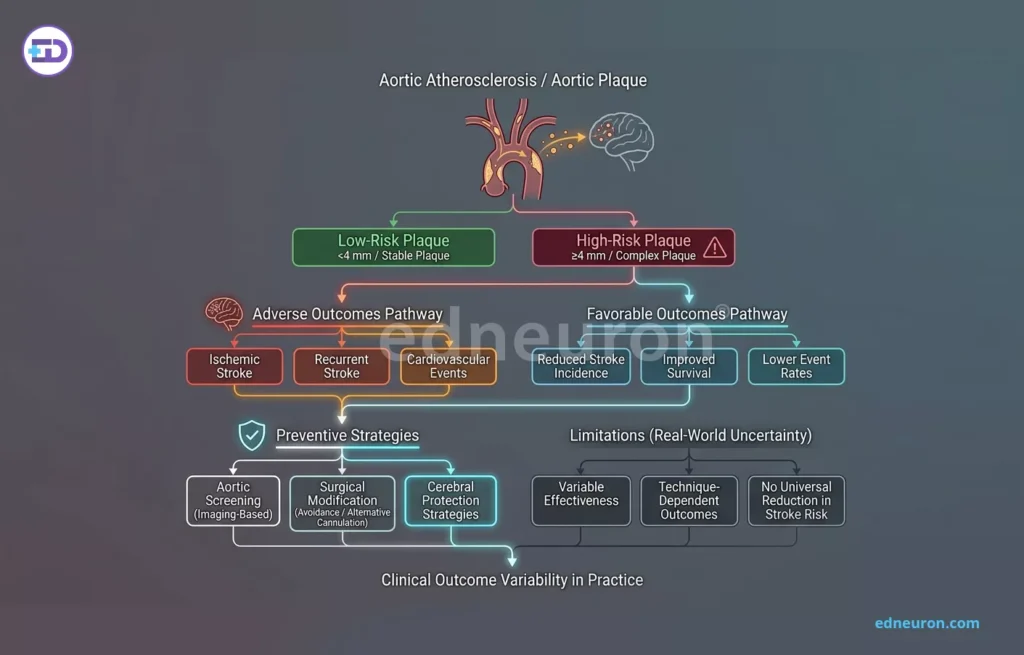
Fig 3: Management strategy and clinical outcomes in the treatment of atherosclerotic plaque.
Conclusion
Aortic atherosclerosis is not a binary condition but a spectrum that demands a tailored surgical response. What is required is a shift from routine protocols to a high-fidelity diagnostic model where the choice of cannulation and clamping is dictated by the specific topography of intimal disease. Ultimately, the goal is to navigate the hostile aorta with a strategy that prioritizes the brain as much as the heart, acknowledging that the most elegant surgical repair is of little value if the cost is a debilitating embolic event.
References
- Khalpey, Z., et al. (2021). Intimal aortic atherosclerosis in cardiac surgery: Surgical strategies and outcomes. Journal of Cardiothoracic Surgery, 16(1), 1–10.
- Malas, M. B., et al. (2020). Endovascular versus open repair of common femoral artery atherosclerosis: A systematic review and meta-analysis. Journal of Vascular Surgery, 72(6), 2174–2185.
- Soylu, E., et al. (2014). Coronary endarterectomy with coronary artery bypass grafting: A meta-analysis of over 100,000 patients. Interactive Cardiovascular and Thoracic Surgery, 19(3), 428–437.
- Rehman, S. M., et al. (2024). Open versus minimally invasive coronary artery bypass grafting for atherosclerotic coronary disease: A systematic review. Journal of Clinical Medicine, 14(5), 147.
- Khan, M. A., et al. (2019). Hybrid surgical and endovascular management of systemic atherosclerosis: A case-based review. International Journal of Clinical Cardiology, 6(158), 1–5.
- Rashid, M., et al. (2023). Medical and surgical management of symptomatic and asymptomatic carotid artery stenosis: A comprehensive review. Cureus, 15(8), e173388.
- Sharma, A., et al. (2023). Exploring the arterial realm: A comprehensive review of vascular surgery in atherosclerotic disease. Journal of Vascular Medicine & Surgery, 11(2), 1–8.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



