

Introduction
Chronic kidney disease in diabetic patients is traditionally characterized by the presence of albuminuria, with progression from microalbuminuria to macroalbuminuria accompanied by reduced glomerular filtration and its sequential progression to ESKD (End-Stage Kidney Disease). Afkarian M et al. 2016 study reports that among the diabetic patients, a paradigm shift from albuminuric CKD to non-albuminuric CKD was witnessed with decreased prevalence of albuminuria (20.8% [95% CI, 16.3%-25.3%] in 1988-1994 to 15.9% [95% CI, 12.7%-19.0%] in 2009-2014-adjusted prevalence ratio, 0.76 [95% CI, 0.65-0.89]; P < .001 for trend) (refer to the figure below). This shift reflects how the current Mogensen staging standards, which have governed both screening protocols and therapeutic trial design for decades, ignore an upcoming large subset of patients. This non-albuminuric DKD (NA-DKD) phenotype, defined as
- Estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m²-in the absence of urinary albumin-to-creatinine ratio [UACR] <30 mg/g and macroalbuminuria defined as a urine ACR of 300 mg/g or greater.
This is increasingly recognized across large epidemiological cohorts, demanding a fundamental re-evaluation of how diabetic renal disease is defined, detected, and treated.
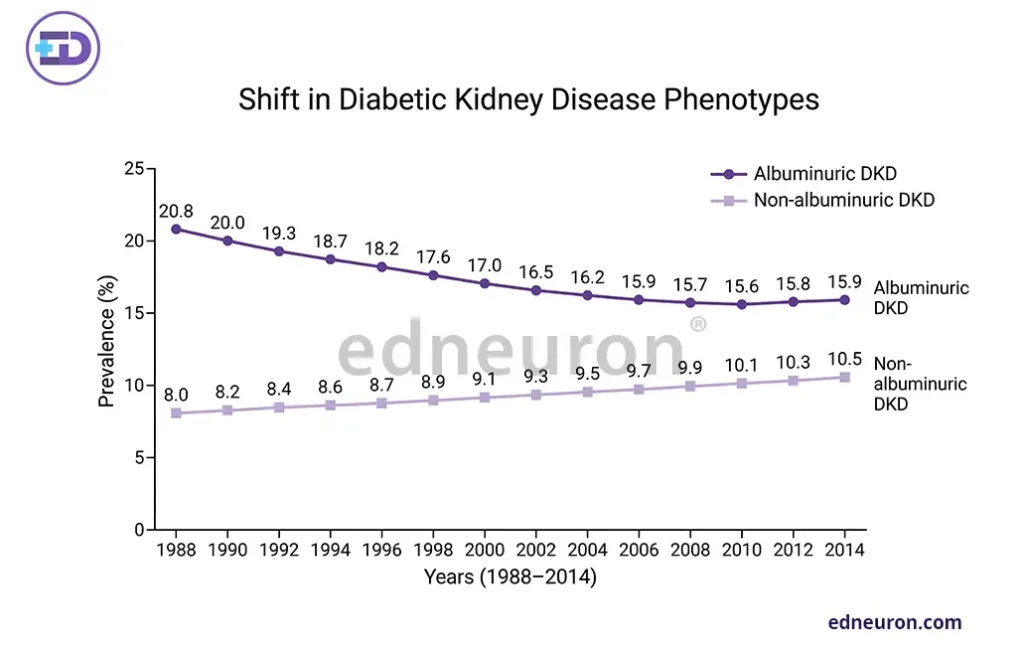
Fig 1: Increasing trend in the prevalence of non-albuminuric DKD over the years (1988-2014).
Epidemiology
Population-based analyses consistently demonstrate that NA-DKD constitutes a substantial proportion of DKD. Data from the NHANES estimate that between 20% and 40% of T2D patients with CKD are present, with some series reporting even higher proportions among elderly individuals. These individuals are predominantly older, female, and hypertensive, and tend to have a more favorable metabolic profile with lower HbA1c and longer diabetes duration, and a slower decline in eGFR compared to their albuminuric counterparts, a demographic signature that carries its own prognostic implications.
Pathophysiology
The basis of NA-DKD is distinctly heterogeneous and likely multifactorial, diverging meaningfully from the supposed glomerular leak that causes albuminuria. Renal biopsy series, limited in number but informative, reveal that NA-DKD patients exhibit less severe glomerulosclerosis and instead manifest tubulointerstitial fibrosis, arteriolar hyalinosis, and arteriosclerosis leading to ischemic nephropathy. Macroangiopathic ischemia, more than microvascular causes, may precipitate tubular atrophy without the appreciable glomerular leak, i.e., albuminuria.
Repeated subclinical acute kidney injury (AKI) likely acts synergistically in tubular damage, particularly in older patients, often implicated as a major driving force for CKD.
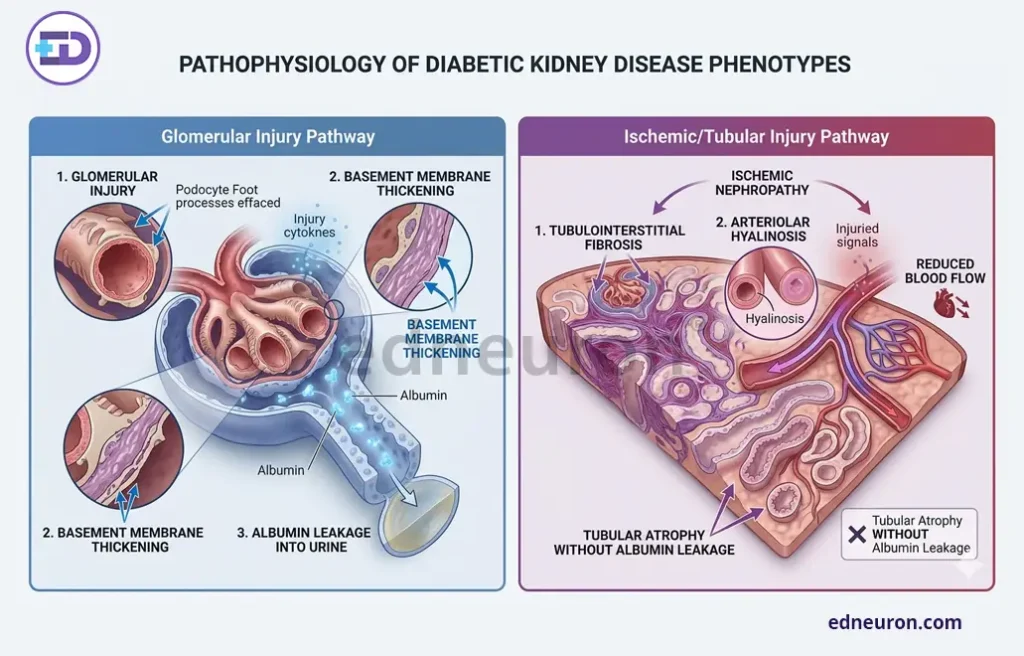
Fig 2 : Pathophysiological Pathways of Diabetic Kidney Disease (DKD): Glomerular vs Tubulointerstitial Phenotypes.
Diagnostic Challenges and Biomarker Gaps
Current clinical guidelines continue to embed the diagnosis of NA-DKD in UACR, putting it squarely in the blind spot. Although eGFR monitoring is recommended, it is often interpreted in isolation, without formal CKD staging for patients below the albuminuria threshold. We do have certain new markers, such as NGAL (neutrophil gelatinase-associated lipocalcin) and KIM-1, which reflect the earliest rise in serum levels when the tubular system is injured. Nevertheless, none have been validated in prospective trials or integrated into clinical decision pathways as primary investigation for acute kidney injury. The ongoing absence of a consensus biomarker panel for non-albuminuric renal pathology remains a critical evidence gap, necessitating improvements in phenotyping NA-DKD.
Prognosis and Cardiovascular Risk
Despite a comparatively favorable metabolic profile and better Cardiovascular outcomes, NA-DKD is not a benign entity. Compared with DKD with marked albuminuria and reduced eGFR, it has slower progression and less severe cardiovascular outcomes. The Renal Insufficiency and Cardiovascular Events (RIACE) study reported that the risk of CV mortality was higher in individuals with nonalbuminuric DKD and eGFR < 45 mL/min/1.73 m2 compared to those with albuminuria alone. NA-DKD patients demonstrate elevated rates of major adverse cardiovascular events (MACE). One reason for this shift toward non-albuminuria is the use of RAAS inhibitors, which, by dilating the efferent arteriole, reduce intrarenal pressure, thereby masking albuminuria. A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO), however, reports that there is underprescription of RAASi and SGLT2 inhibitors. This brings us to two competing, distorting thoughts.
- Undertreatment – marked albuminuria with worse CV outcomes.
- Use of RAASi- masking of albuminuria with eGFR (importance of eGFR in risk stratification in isolation) in DKD.
Without phenotype-stratified trials, therapeutic recommendations for NA-DKD rest on extrapolation rather than direct evidence.
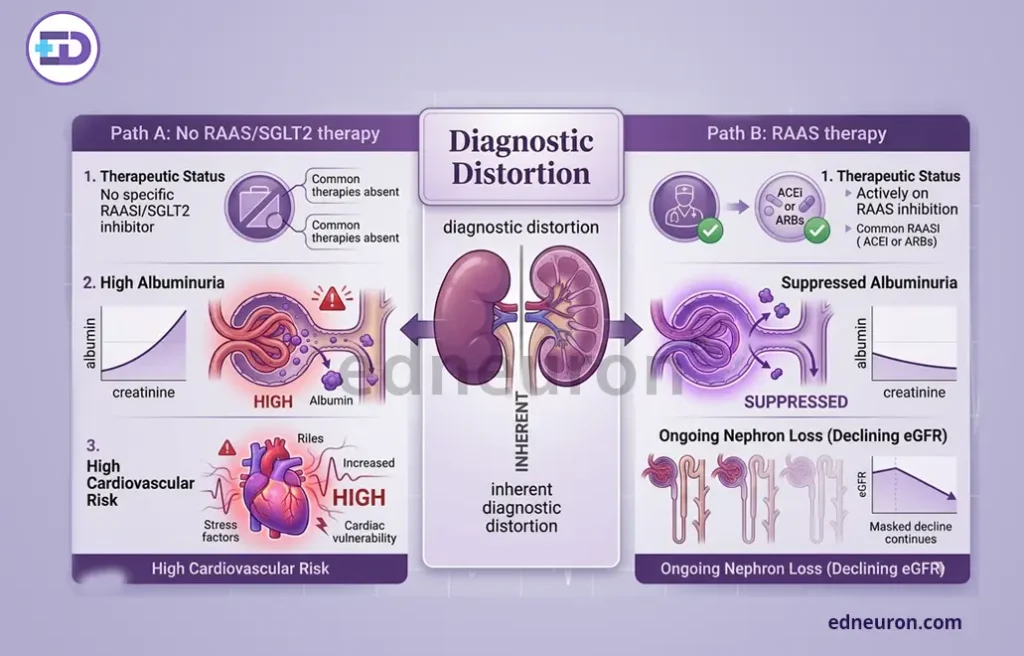
Fig 3 : The diagnostic distortion resulting from RAASi is due to decreased intrarenal pressure, reducing albuminuria in the presence of concomitant tubulointerstitial injury and declining eGFR.
Conclusion
Non-albuminuric DKD represents a coherent, epidemiologically substantial, and clinically consequential renal phenotype that is fundamentally incompatible with albuminuria-centric DKD models. Its unique pathophysiology, dominated by tubulointerstitial injury, ischemic nephropathy, and possible RAAS-mediated masking of glomerular damage, demands distinct diagnostic frameworks and dedicated therapeutic trials. The field urgently requires prospective validation of tubular biomarkers, revision of screening algorithms to incorporate eGFR trajectory alongside UACR, and inclusion of NA-DKD strata in future outcome trials. Until these gaps are addressed, a clinically important patient population will remain systematically underdiagnosed and inadequately treated.
References
- Afkarian M, Zelnick LR, Hall YN, et al. Clinical Manifestations of Kidney Disease Among US Adults With Diabetes, 1988-2014. JAMA. 2016.
- D’Marco L, Guerra-Torres X, Viejo I et al. Non-albuminuric Diabetic Kidney Disease Phenotype: Beyond Albuminuria. touchREV Endocrinol. 2022 Nov PMID: 36694889.
- Janota-Sosińska O, Mantovani M, Irlik K et al. Diabetic kidney disease phenotypes and the risk of cardiovascular events: The Silesia Diabetes-Heart Project. Cardiovasc Diabetol. 2025 Jul PMID: 40739504.
- Yokoyama H, Araki SI, Kawai K et al. JDDM Study Group. The Prognosis of Patients With Type 2 Diabetes and Nonalbuminuric Diabetic Kidney Disease Is Not Always Poor: Implication of the Effects of Coexisting Macrovascular Complications (JDDM 54). Diabetes Care. 2020 PMID: 32144168.
- Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 2012 Mar PMID: 22113526.
- Limonte CP, Gao X, Bebu I et al. DCCT; EDIC Research Group. Associations of Kidney Tubular Biomarkers With Incident Macroalbuminuria and Sustained Low eGFR in DCCT/EDIC. Diabetes Care. 2024 Sep PMID: 38484321.
- Penno G, Solini A, Orsi E, et al. Non-albuminuric renal impairment is a strong predictor of mortality in individuals with type 2 diabetes: the Renal Insufficiency and Cardiovascular Events (RIACE) Italian multicentre study. Diabetologia. 2018.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



