

Introduction
The way we understand central nervous system (CNS) demyelination has changed significantly, shifting from the broad term “Devic’s disease” to the more specific Neuromyelitis Optica Spectrum Disorder (NMOSD). The discovery of the aquaporin-4 antibody (AQP4-ab) has improved diagnostic precision, but challenges remain. Many patients are still “double seronegative,” and MOG-antibody-associated disease (MOGAD) has emerged as a separate condition. This article examines the challenges of diagnosing and treating patients within this precision gap.
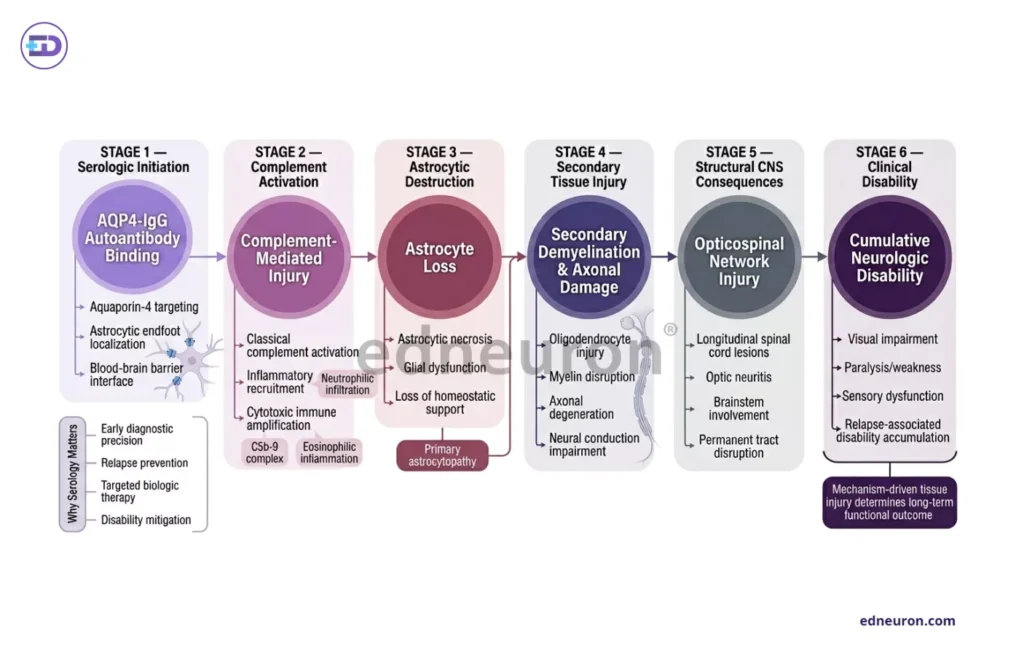
Fig 1 : AQP4-IgG-mediated astrocytic injury initiates complement-driven neuroinflammation, leading to secondary demyelination and cumulative neurologic disability in NMOSD.
The Astrocytic Siege: How Mechanisms Reflect Disability
Unlike multiple sclerosis (MS), which mainly involves T-cell attacks on oligodendrocytes, AQP4-positive NMOSD is an autoimmune disease that targets astrocytes. Here, harmful IgG antibodies bind to AQP4 water channels on astrocyte end-feet, which are grouped in specific patterns. This triggers the complement system, leading to cell damage and the formation of the membrane attack complex (MAC), which often causes severe, sometimes permanent, tissue loss.
This aggressive process explains why NMOSD causes disability in sudden steps after attacks, instead of gradually getting worse over time. MS patients often recover well from early relapses, but a single NMOSD attack can cause permanent blindness or paralysis. This raises a key question: how should we treat patients who clearly present with NMOSD symptoms but test negative for antibodies?
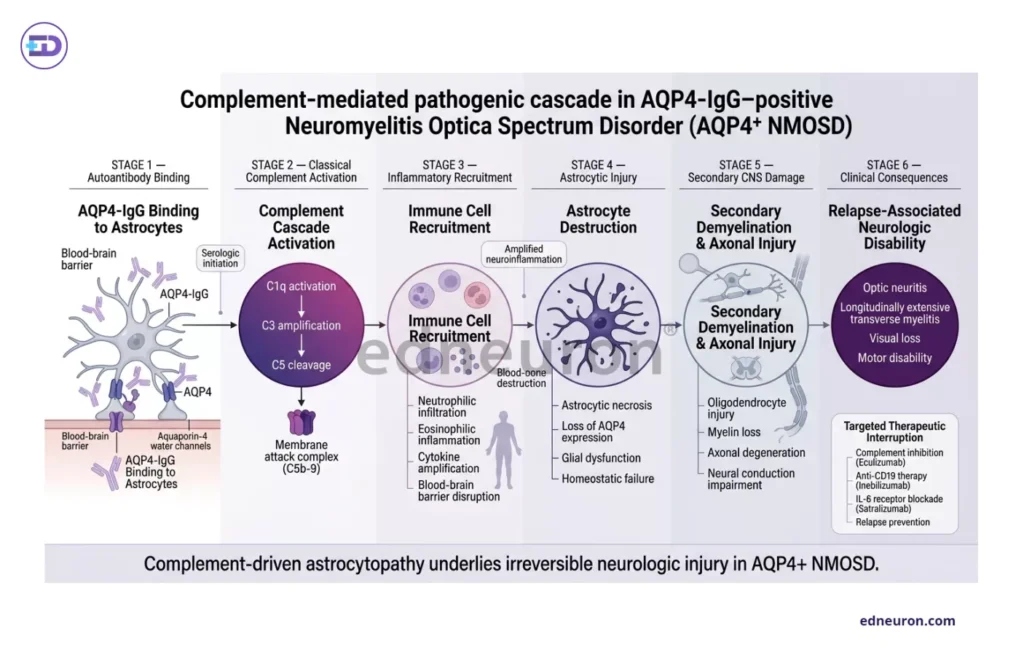
Fig 2 : AQP4-IgG–mediated complement activation drives astrocytic destruction, secondary demyelination, and progressive neurologic disability in NMOSD.
The Diagnostic Challenge: Antibodies, Biomarkers, and Similar Conditions
The discovery of MOGAD has made diagnosis more complex because it often resembles NMOSD, with severe optic neuritis or long spinal cord inflammation, but it targets a different protein on oligodendrocytes rather than astrocytes, meaning doctors need to interpret test results carefully. For example, serum glial fibrillary acidic protein (sGFAP) is much higher during AQP4-positive attacks, indicating direct astrocytic damage, but remains lower in MOGAD and MS.
Imaging helps distinguish these conditions. AQP4-positive lesions usually appear in the center of the spinal cord and look “bright spotty” on T2 MRI scans. MOGAD lesions often show the “H-sign,” indicating they are located in the spinal gray matter. Still, doctors need to watch for “double-negative” NMOSD, in which neither AQP4 nor MOG antibodies are detected, suggesting there may be other causes we have not yet identified.
The Diagnostic Challenge: Antibodies, Biomarkers, and Similar Conditions
Long-term treatment has shifted from general immunosuppressants such as azathioprine and mycophenolate to more targeted biologic drugs that block specific disease pathways. Three main strategies have recently changed how we treat NMOSD:
- Complement Inhibition: Eculizumab prevents cleavage of C5, thereby preventing the membrane attack complex (MAC) from damaging astrocytes. This leads to a 94% reduction in relapse risk.
- B-Cell Depletion: Inebilizumab targets CD19+ B-cells, including the AQP4-ab-producing plasmablasts that rituximab may miss.
- IL-6 Receptor Blockade: Satralizumab and tocilizumab block IL-6 signaling, which helps plasmablasts survive and affects the blood-brain barrier.
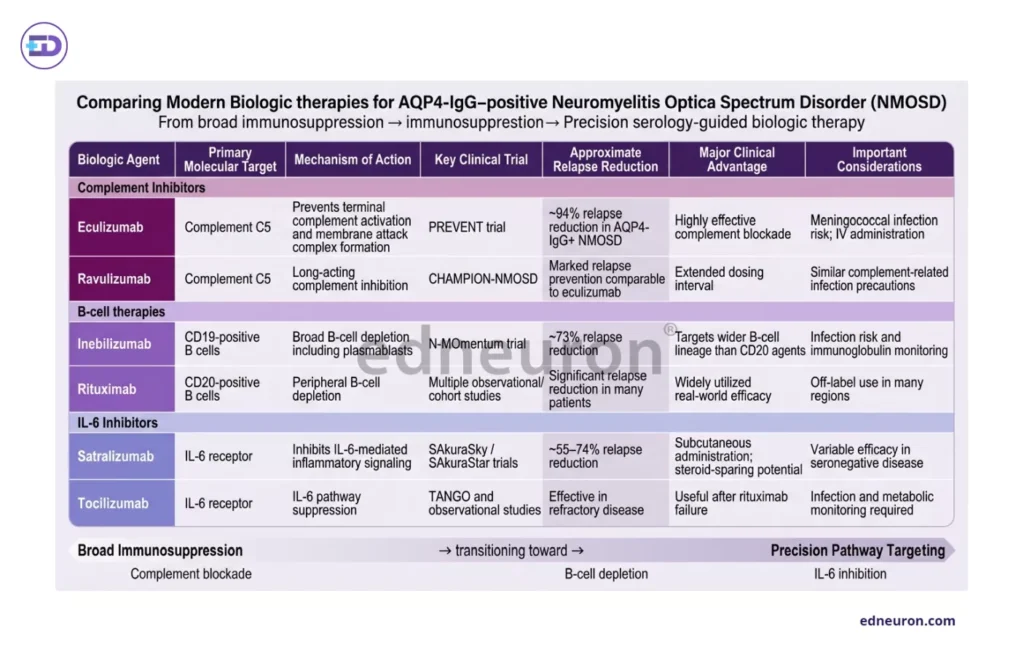
Table 1 : Comparative mechanisms and efficacy profiles of modern biologic therapies targeting complement, B-cell, and IL-6 pathways in AQP4-IgG–positive NMOSD.
Another challenge is weighing the risks and benefits of these treatments. Eculizumab is very effective, but patients must always be monitored for meningococcal sepsis, which affects who can safely use this drug.
Conclusion: Moving Toward a Multimodal Approach
Treating NMOSD is no longer just a matter of trying different general immunosuppressants. Because the precision gap in antibody testing remains, we need a clear, structured approach that uses multiple methods:
- Early Antibody Stratification: Using cell-based tests is essential for telling AQP4-positive NMOSD apart from MOGAD.
- Biomarker Integration: sGFAP and NfL can help quantify the severity of an attack and track tissue damage that may not present with symptoms.
- Therapeutic Tailoring: Selecting biologics based on serostatus, as complement inhibitors have no proven efficacy in AQP4-negative or MOGAD cases.
The main goal is to bridge the gap between what we know at the molecular level and how we treat patients, so that everyone receives the targeted care they need.
References
- Huda S, Whittam D, Bhojak M, Chamberlain J, Noonan C, Jacob A. Neuromyelitis optica spectrum disorders: pathophysiology and therapeutic strategies. J Neuroinflammation. 2021;18(1):208. doi:10.1186/s12974-021-02249-1. PMID: 34446005.
- Flanagan EP, Juryńczyk M, Fujihara K, Palace J. MOG CNS autoimmunity and MOGAD. Neurol Neuroimmunol Neuroinflamm. 2024;11(2):e200275. doi:10.1212/NXI.0000000000200275. PMID: 38324562.
- Li Y, Wang J, Chen Z, Zhang Y. Soluble biomarkers for neuromyelitis optica spectrum disorders: a mini review. Front Neurol. 2024;15:1381188. doi:10.3389/fneur.2024.1381188. PMID: 38729876; PMCID: PMC11137173.
- Dubey D, Sechi E, Krecke KN, Chen JJ, Pittock SJ, Weinshenker BG, et al. Myelitis features and outcomes in CNS demyelinating disorders: comparison between multiple sclerosis, MOGAD, and AQP4-IgG-positive NMOSD. Front Neurol. 2022;13:1011579. doi:10.3389/fneur.2022.1011579. PMID: 36405211; PMCID: PMC9676369.
- Solomon AJ, Watts R, Ontaneda D. Visualizing the central nervous system: imaging tools for multiple sclerosis and neuromyelitis optica spectrum disorders. Front Neurol. 2020;11:450. doi:10.3389/fneur.2020.00450. PMID: 32508762; PMCID: PMC7311777.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



