

The Admission That Looks Familiar At The Psychiatric Dept.
She is twenty-two years old, a university student with prodromal flu-like illness but no psychiatric history, brought in by her friends after three weeks of escalating aberrant savagery, agitation, paranoid beliefs that her food is being poisoned, schemes of her murder, and auditory hallucinations of voices narrating her movements. The on-call psychiatrist completes the assessment and concludes what seems like the most obvious presentation- first episode of psychosis. An antipsychotic is prescribed. A crisis bed is arranged. By the second night, she cannot sustain a conversation for more than two minutes. Her sleep is fractured and bizarre, she is awake at 3 a.m., staring, moving her mouth without speaking. Her heart rate climbs to 122. The nurses chart ‘agitation’ and increase the sedation. Then, on the third morning, she goes into a tonic-clonic seizure.
The psychiatrist who first assessed her was not wrong to consider first-episode psychosis. What the trickery of presentation was that in a young woman with no prior history, rapid psychiatric deterioration accompanied by fluctuating consciousness, autonomic instability, and vegetative tachycardia does not belong to psychiatry until neurology has been formally excluded. Orofacial dyskinesias: stereotyped lip-smacking, tongue protrusion, and jaw movements may be dismissed as medication side effects or anxiety. Fluctuating consciousness, the waxing and waning of orientation across a single ward round or even during a single assessment, may be charted as ‘variable engagement.’ Autonomic instability: tachycardia, labile blood pressure, hyperhidrosis, and urinary incontinence may be attributed to anxiety or the anticholinergic burden of the antipsychotic itself. Catatonia may be interpreted as an extreme manifestation of psychotic withdrawal. Each individual sign, evaluated in isolation, fits somewhere within a psychiatric explanation. Evaluated together, and in temporal sequence, they constitute a syndromic fingerprint that Dalmau and colleagues first systematically characterized in their landmark 2008 description of anti-NMDA receptor encephalitis: psychiatric onset, followed by seizures, movement disorder, autonomic instability, and if untreated, progressive impairment of consciousness.
A Differential That Cannot Stop at Psychiatry
The differential diagnosis of acute psychosis in a young adult is nowhere near narrow. Schizophrenia spectrum disorder is the most recognizable form and the most dangerous one to apply prematurely. Substance-induced psychosis, particularly cannabis, stimulants, and novel psychoactive agents, must be actively pursued. Delirium from metabolic, infective, or toxic causes can produce hallucinations and agitation, and its cardinal feature, fluctuating consciousness, is precisely the feature most often under-documented in acute psychiatric assessments. Autoimmune encephalitis, particularly anti-NMDA receptor encephalitis, sits within this differential not as a rare guest but as a systematically underrecognized condition, perhaps because such patients with a psychotic prodrome present first to a psychiatrist and not a neurologist.
An Immune Attack That Speaks Fluent Psychiatry
The neurobiology of anti-NMDA receptor encephalitis resolves what might otherwise seem like an implausible coincidence- that an autoimmune process would produce, with such fidelity, a syndrome indistinguishable from schizophrenia. IgG antibodies targeting the NR1-NR2 heteromers of the NMDA receptor bind to synaptic and extrasynaptic receptors, triggering antibody-mediated internalization and a reversible but functionally catastrophic reduction in NMDA receptor density. These are documented to be well associated with ovarian teratomas, viral infections (though direct viral pathology is unlikely), and post-vaccination. Since most studies indicate the absence of viruses in brain biopsies and CSF, it remains a contentious debate whether such viral attack primes the early immune response or facilitates antibody entry into the CNS via BBB dysfunction.
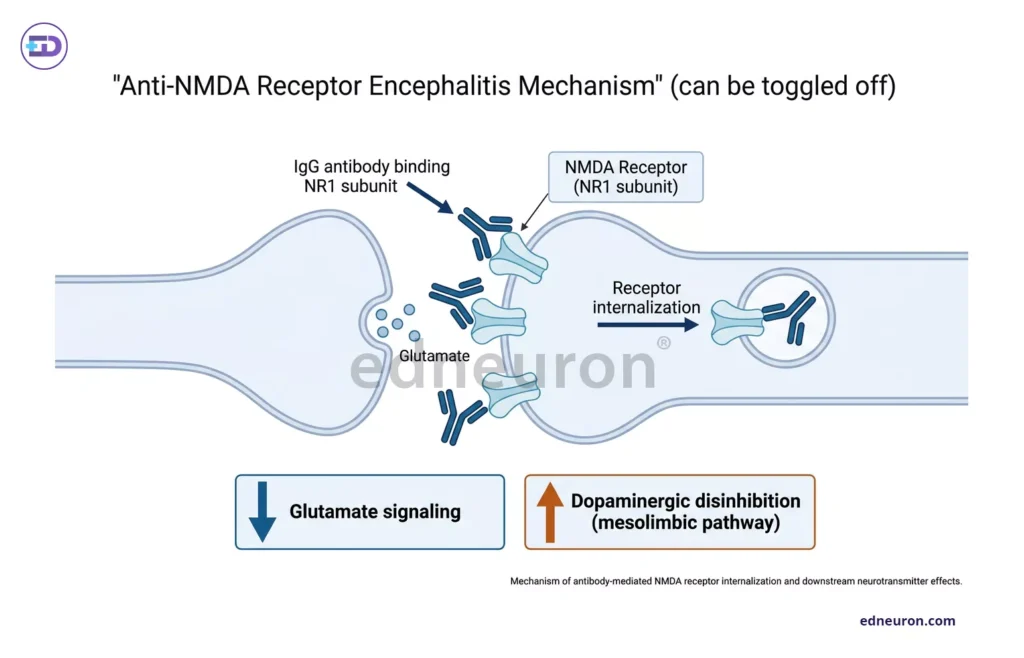
Fig 1: Mechanism of anti-NMDA antibodies- the binding of these antibodies results in the reversible internalization of these receptors, causing disinhibition of mesolimbic pathways.
The downstream consequence is disinhibition of mesolimbic dopaminergic pathways producing a neurochemical state that approximates the dopamine dysregulation model of schizophrenia with such high fidelity and renders the demarcation sublime. Psychosis appears early because glutamate-dopamine dysregulation is the first consequence of receptor loss. Seizures, movement disorders, hypoventilation, and autonomic instability accompany the antibody-mediated glutaminergic disruption umbra, which seizes the cortical, subcortical, and autonomic circuits. This is not schizophrenia. It is immune-mediated synaptic failure that borrows the language of psychiatry for its prelude. The distinction matters because the treatment- immunotherapy, not antipsychotics, targets the antibody, not the symptom. However, such reliance on antibody testing and on responses to immunotherapy risks delaying diagnosis. The 2016 diagnostic criteria published by Graus et al. provided the most operationally useful framework: Diagnosis can be made when all three of the following criteria have been met:
- Subacute onset (rapid progression of less than 3 months) of working memory deficits (short-term memory loss), altered mental status, or psychiatric symptoms.
- At least one of the following.
- New focal CNS findings
- Seizures not explained by a previously known seizure disorder
- CSF pleocytosis (white blood cell count of more than five cells per mm3)
- MRI features suggestive of encephalitis
- Reasonable exclusion of alternative causes (CNS infections, HSV encephalitis, metabolic encephalopathies, etc.)
Many patients being AE seronegative also emphasize comprehensive history-taking, accurate clinical examination, and supportive diagnostic tests (such as MRI, inflammatory CSF parameters, and EEG). CSF antibodies might also be absent because the brain acts as an immunoprecipitator, and such brain-binding antibodies may not be readily detected in assessments. It is also true that EEG findings in such cases are rarely specific when the presentation is ambiguous; however, some cases of NMDA Encephalitis present with an extreme delta brush (Fig 2), a specific phenomenon, as a clue to the diagnosis. The framework is deliberately hierarchical because treatment cannot wait for laboratory confirmation when clinical deterioration is ongoing, thereby expediting stepwise diagnostic decision-making.
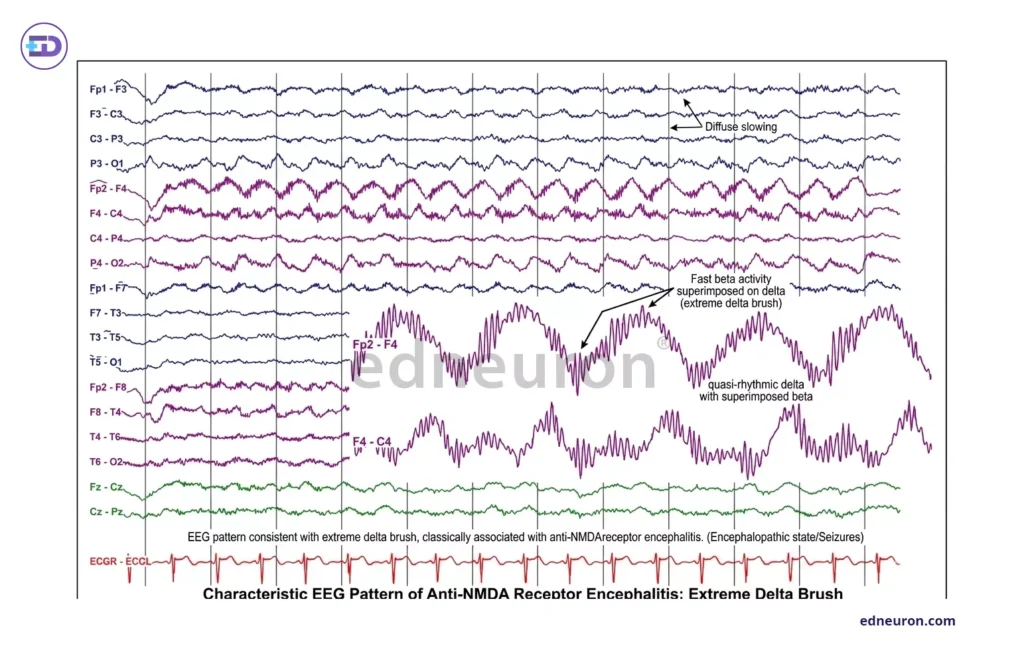
Fig 2 : EEG- extreme delta brush- suggestive of autoimmune encephalitis. High-amplitude, rhythmic delta waves (1–3 Hz) form the slow-wave background. Superimposed on these slow oscillations are bursts of fast beta-frequency activity (20–30 Hz), creating a morphology reminiscent of the “delta brush” pattern seen in premature neonatal EEG, but with exaggerated amplitude and persistence, hence termed extreme delta brush.
What Primary Psychosis Does Not Do- AE In Psychiatric Patients
In a structured study of clinical warning signs, Herken and Prüss identified features that favor autoimmune encephalitis over primary psychiatric illness, thus reducing the time from symptom onset to diagnosis by 58%.
- Rapid progression over days to weeks
- Fluctuation in the level of consciousness during a single assessment
- New-onset seizures in a patient without epilepsy
- Orofacial or limb dyskinesias
- Autonomic instability not explained by medication
- Catatonia, particularly when it emerges without a clear affective or psychotic context.
When such red flags are explicitly identified, a prompt neurological investigation should be mandated, regardless of the apparent psychiatric clarity of the presentation. Schizophrenia does not cause fluctuating consciousness. It does not cause tachycardia and blood pressure lability, nor does it cause orofacial stereotypies in a previously neurologically intact young person. When these features appear, the diagnosis of primary psychosis should be held with uncertainty, not confidence.
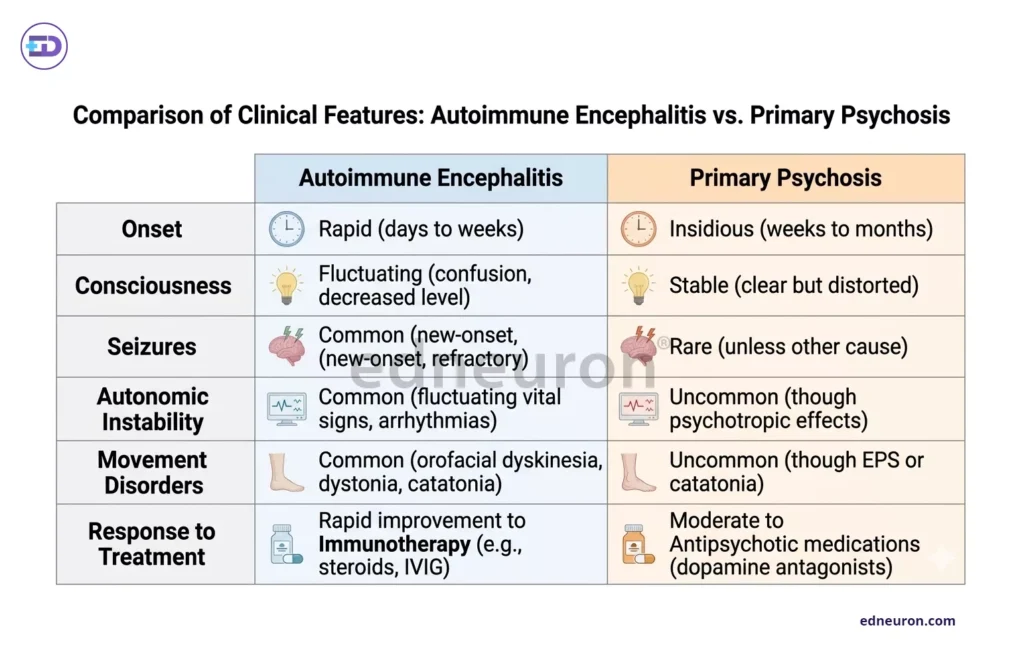
Fig 3 : Tabulated summary of difference between AE and Primary Psychosis.
The Cost of the Wrong Frame
The consequences of diagnostic delay in autoimmune encephalitis are not proportionate to the delay; they are exponential. Titulaer and colleagues’ landmark tertiary center cohort study demonstrated that earlier initiation of immunotherapy as first-line therapy and timely tumor removal as second-line therapy in paraneoplastic cases were independently associated with significantly better long-term outcomes. Conversely, patients diagnosed late required prolonged ICU admission, faced persistent cognitive and functional deficits, and in a meaningful proportion, did not recover. A 2026 prospective first-episode psychosis screening study found at least one death attributable to delayed AE recognition among its cohort- an outcome that is, by definition, preventable if the diagnosis is reached before the disease reaches an irreversible stage. The cost of diagnostic delay is not persistence of symptoms, but progression of disease. Antipsychotics, administered to a patient whose psychosis is driven by antibody-mediated receptor internalization, do not address the mechanism and may mask the neurological evolution, delaying the recognition that the clinical picture is worsening rather than responding.
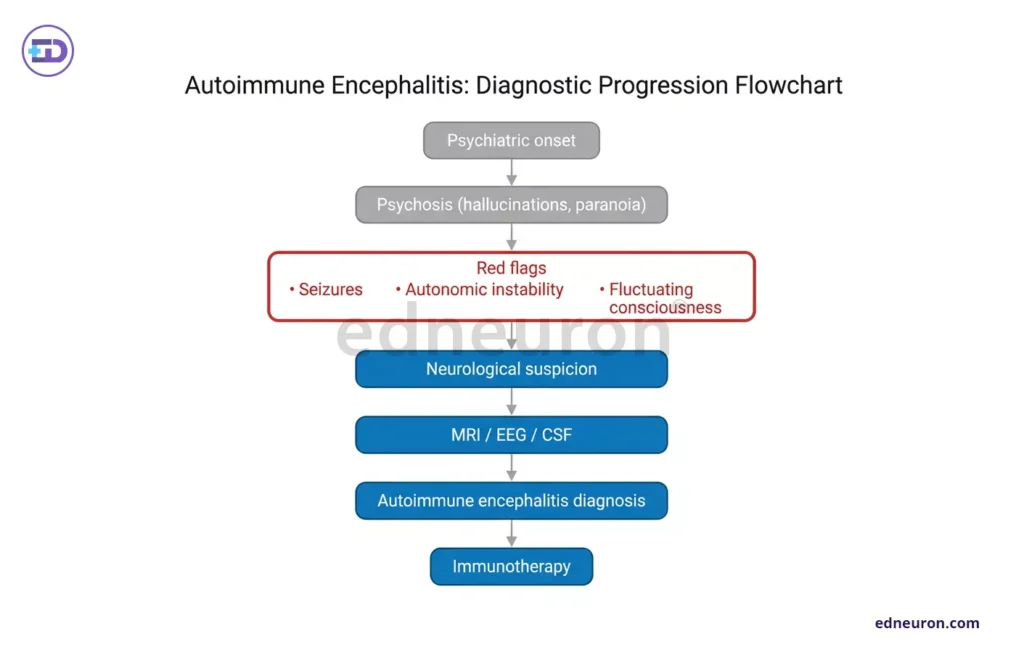
Fig 4 : Evaluation strategy.
Routine Screening and Its Discontents
The evidence of a subset of AE within first-episode psychosis (FEP) populations has generated a legitimate debate about whether antibody screening should become routine practice. The argument for screening rests on the findings that some patients with treatable diseases are being misclassified. The case against or at least for caution, rests on equally important grounds: nonspecific antibody positivity in serum (as opposed to CSF) is common and clinically ambiguous. It risks the mislabeling of primary psychosis with an immunological diagnosis that then drives inappropriate immunosuppression. Seronegative autoimmune encephalitis in which no pathogenic antibody is detected in either serum or CSF further complicates the landscape. A negative result does not exclude the diagnosis when clinical suspicion is high and supportive investigations all point to the same convergent point. Emerging consensus is that the clinical scenario, and contextualizing the presence of red flags, should guide testing.
Conclusion
The brain, when inflamed, does not announce itself with fever or meningism. It can speak the language of psychiatry with disarming fluency, in the voice of paranoia, hallucination, and disorganized thought. The clinical triumph is in being conscientious; first-episode psychosis in a young adult, particularly one with rapid progression, fluctuating consciousness, movement disorder, or autonomic instability, may imply something that isn’t limited to a psychiatric problem. The question, when confronting such a patient, is whether the brain itself is under attack, and whether the window for an immune intervention that could entirely change the illness’s trajectory is still open.
References
- Dalmau J, Gleichman AJ, Hughes EG et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol. 2008 Dec. PMID: 18851928.
- Endres D, Rauer S, Kern W et al. Psychiatric Presentation of Anti-NMDA Receptor Encephalitis. Front Neurol. 2019 Nov. PMID: 31749755
- Graus F, Titulaer MJ, Balu R et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016 Apr; PMID: 26906964.
- Herken J, Prüss H. Red Flags: Clinical Signs for Identifying Autoimmune Encephalitis in Psychiatric Patients. Front Psychiatry. 2017 Feb. PMID: 28261116.
- Titulaer MJ, McCracken L, Gabilondo I et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013 Feb. PMID: 23290630.
- Vera Fominykh, Irina Kovaleva, Ekaterina Aksenova et al. Autoimmune encephalitis in first episode psychosis: Prospective non-interventional longitudinal study in tertiary psychiatric center, Journal of Neuroimmunology, Volume 410, 2026, 578815, ISSN 0165-5728

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



