

Introduction
He no longer hears voices in his head. The persecutory tyrant that had governed his waking hours for the last three years has substantially ebbed like a receding tide. By every standard metric of psychosis control, the clinician reassures- treatment is working. And yet, over the same six weeks that his hallucinations and positive symptoms have quietened, his family has watched him become transparent in the world: he barely speaks, sits motionless for hours, has lost interest in food and conversation, and moves with the deliberate heaviness as if his flesh is leaden and has become someone ancient. His psychiatrist, reviewing the progress notes, sees that the man is improving. His mother, sitting across the consulting room, is describing someone she no longer recognizes as her son.
This paradox, a psychiatrist often recognizes- psychosis subsiding, but the deterioration of the patient is one of the most nuanced parts of schizophrenia management. The familiar narrative of a patient’s progression of the disease’s negative symptoms is not unexpected. Still, the temptation to interpret it as a functional decline inherent and central to schizophrenia’s morbidity, despite treatment, must be resisted. Asking whether it is a siege by the advancing disease or the treatment instituted is crucial in deterring the dangerous assumption.
Careful Interpretation Unravels The Cause
A more extensive examination reveals detailed intricacies and helps reframe the picture.
- The patient’s antipsychotic dose was doubled four weeks ago following an episode of agitation, a clinically reasonable decision at the time.
- However, his physical examination reveals notable facial inexpressiveness, minimal arm swing when he walks, and passive wrist movement with mild cogwheel rigidity.
- He describes feeling as though his thoughts are ‘stuck in mud.’ He is not distressed by this; he is insensitive(absence of drive, not the typical feeling of hopelessness).
These observations collectively help us maneuver through the question of whether this is the natural forward march of schizophrenia’s negative syndrome, or has the treatment introduced the very deficits we are attributing to the disease?
Indistinguishable Primary and Secondary Negative Symptoms
Secondary negative symptoms are phenomenologically identical to primary ones but arise from a distinct, modifiable source and thus are potentially treatable. The various causes of such secondary negative symptoms are:
- Antipsychotic-induced Parkinsonism, characterized by bradykinesia, masked facies, rigidity, and reduced spontaneous movement, is a well-established consequence of D2 receptor blockade and produces a clinical picture mimicking primary negative symptoms on cross-sectional assessment.
- Comorbid depressive disorder– Post-psychotic depression remains common, often presenting with reduced energy, social withdrawal, psychomotor retardation, and diminished speech beingan almost perfect overlap with the negative syndrome.
- Residual positive symptoms, like paranoia, burden the social withdrawal,
- Impoverishing effects of institutional or social deprivation.
The Kirkpatrick–Marder consensus through the MATRICS initiative reinforced this heterogeneity, establishing that
- Avolition: reduced motivation
- Anhedonia: reduced ability to experience pleasure
- Asociality: a lack of interest in social engagement
- Blunted affect: increased emotional inexpressiveness
- Alogia: reduced speech expression
By virtue of temporal correlation, motor signs, and recent dose escalation, antipsychotic drug-induced Parkinsonism is indeed a credible differential, but depression deserves equal attention because it carries distinct therapeutic implications and significant mortality risk.
We cannot simply exclude depression on the basis of unremarkable subjective expression of distress, as such reduced emotional reactivity may mask dysphoria.
Psychiatric rating instruments, including the PANSS negative subscale and the SANS, quantify avolition, affective blunting, and alogia, but they do not and cannot determine causation. A score of 25 on the PANSS negative subscale tells the clinician how much, but not why. How can the clinician differentiate whether this is an extension of the primary illness or a result of treatment?
Primary negative symptoms, the enduring, antecedent syndrome of the deficit subtype remains possible, but they represent a diagnosis of exclusion rather than a default assumption.
The Dopamine Paradox
This dilemma stems from the very distinct neurocircuitry of dopamine systems in the brain. The dopamine hypothesis helps us understand this phenomenon. Elevated striatal dopamine and its release in the mesolimbic areas drive the salient features of non-deficit schizophrenia, resulting in hallucination, delusions, and paranoia. D2 blockade by antipsychotic drugs alleviates such positive symptoms in the mesolimbic areas. Conversely, the mesocortical projections to the prefrontal cortex, which are responsible for motivational drive, emotional regulation, and executive functioning, take a major hit due to relative dopamine hypofunctionality. This anatomical divergence creates an inherent pharmacological tension and reflects the limited therapeutic efficiency of traditional antipsychotic drugs. Nigrostriatal D2 blockade produces Parkinsonism, and hypofunctioning mesocortical pathway leads to blunted motivation, flattened affect, and impairing the reward anticipation processes. This is not a pharmacological failure; it is a predictable consequence of imprecise circuit targeting, and it demands clinical vigilance proportionate to its frequency.
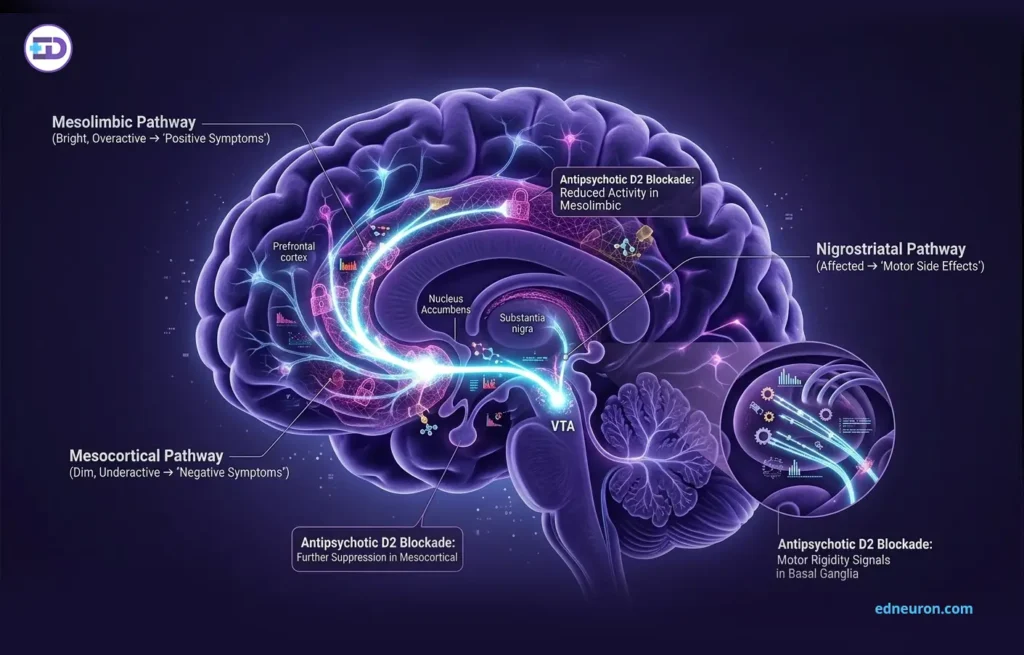
Fig 1: Effect on Dopamine Circuits.
Discriminating Etiology
- Temporal relationship to medication changes is the most actionable clue in differentiating the etiology: symptom onset or worsening following a dose increase or switch to a higher D2-affinity agent strongly implicates a drug effect. This can potentially be helped by reducing the dose. Motor signs: rigidity, cogwheel phenomenon, reduced arm swing, hypomimia favor extrapyramidal syndrome and are not features of primary negative symptoms.
- Subjective dysphoria, guilt, expressed hopelessness, and anhedonia with preserved reactive capacity favor a depressive etiology. An insidious, treatment and secondary intervention independent, antecedent course present before the first psychotic episode and persistent through periods of psychosis remission is the hallmark of the deficit syndrome.
A patient whose psychosis is controlled but who cannot sustain employment, maintain relationships, or experience motivation is not, by any meaningful definition, recovering.
The Cost of Diagnostic Inertia
A clinician who interprets extrapyramidal deterioration as negative symptom progression without considering that the debilitation can be a potential side effect may logically and disastrously escalate the antipsychotic dose, intensifying the very mechanism producing the decline. This therapeutic inertia also risks withholding an effective intervention for a concomitant comorbid depression that might remain undetected. It is at this stage that precise re-evaluation by examining the medication history, performing a focused motor examination, screening for mood disorder, and reassessing the temporal architecture of the patient’s deterioration relative to treatment changes can prove to be most beneficial.
When Progression Is Real?
Intellectual honesty requires not only conscientiousness amidst the skepticism but also acknowledging that the primary negative symptom, i.e., deficit schizophrenia that antedates and persists independent of psychotic episodes, depression, and medication effects, represents a genuine biological subtype. Studies have shown that not only is the neurological profile distinct, but unfortunately, it is also associated with worse functional outcomes and reduced treatment response. So clinicians must not supplant the possibility of deficit schizophrenia with secondary symptoms and vice versa. The task is to structure and systematically exclude secondary causes before accepting that a patient’s deterioration reflects primary illness progression. Even then, the therapeutic response is not passive resignation; it shifts toward functional rehabilitation, psychosocial intervention, and consideration of add-on strategies, because after all, pharmacology alone has shown to have a limited impact on the primary negative syndrome.
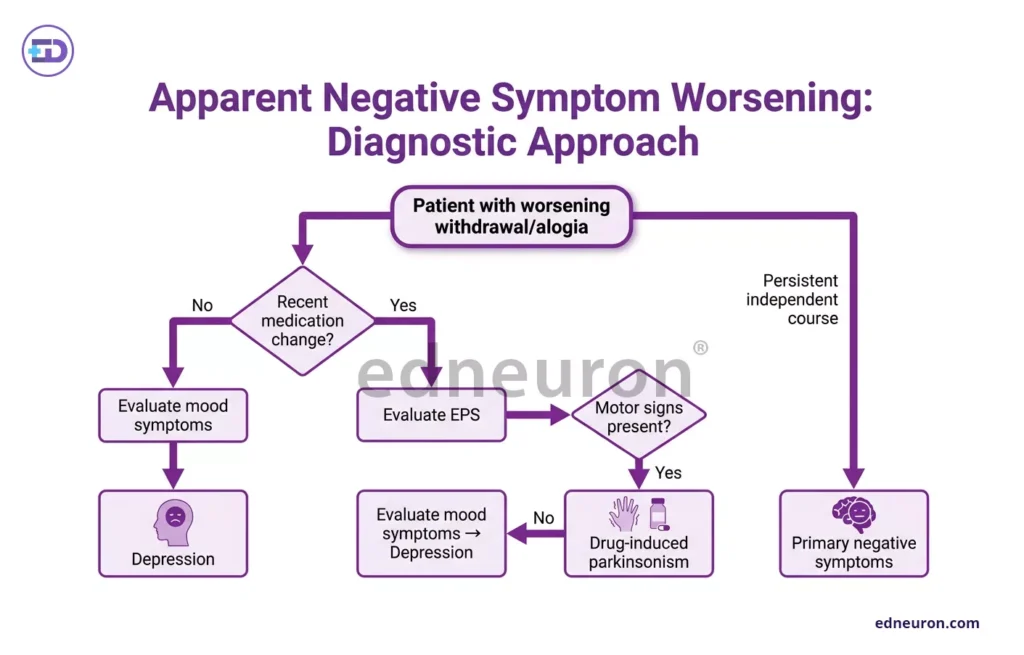
Fig 2: Evaluation strategy.
Conclusion
When a patient with schizophrenia becomes quieter, more withdrawn, morose, and less permeable to the world, the question is not what is progressing, but why. The architecture of dopamine circuits, the paradoxical effect of D2 blockade, and the despondency of depression conspire to one of the most cerebral treacherous presentations in psychiatry. Rating scales can surely measure the magnitude of what is happening, leaving the answer to why to us, the clinicians. The patient in our vignette deserves more than just a perpetual increase in dose and a seemingly never-ending cycle of medication. He deserves a clinician who pauses long enough to ask whether the silence that feeds like hunger on the voice within him is Cerberus in the form of his illness, a dire consequence of his treatment, or an abyss of depression that no one dares to cross.
References
- Kirkpatrick B, Galderisi S. Deficit schizophrenia: an update. World Psychiatry. 2008 OcPMID: 18836581.
- Kirkpatrick B, Fenton WS, Carpenter WT Jr, Marder SR. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr Bull. 2006;32(2):214–219.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



