

Introduction
When clinicians encounter a patient with positive formal thought disorder (FTD), they often see “schizophasia,” a chaotic speech pattern that raises an important neurobiological question: Is this due to a problem in the main language network or to a broader breakdown in the brain’s executive functions? Traditionally, clinicians have seen “word salad” as a language issue, but new connectome-based predictive modeling shows it is not just a local problem. Instead, it points to “cognitive dysmetria,” a condition characterized by widespread disruptions in connections between the frontal, temporal, and thalamic regions. This highlights a key debate: does FTD stem from temporal lobe dysfunction (the dyssemantic hypothesis) or from a failure of higher-level integration (the dysexecutive hypothesis)?
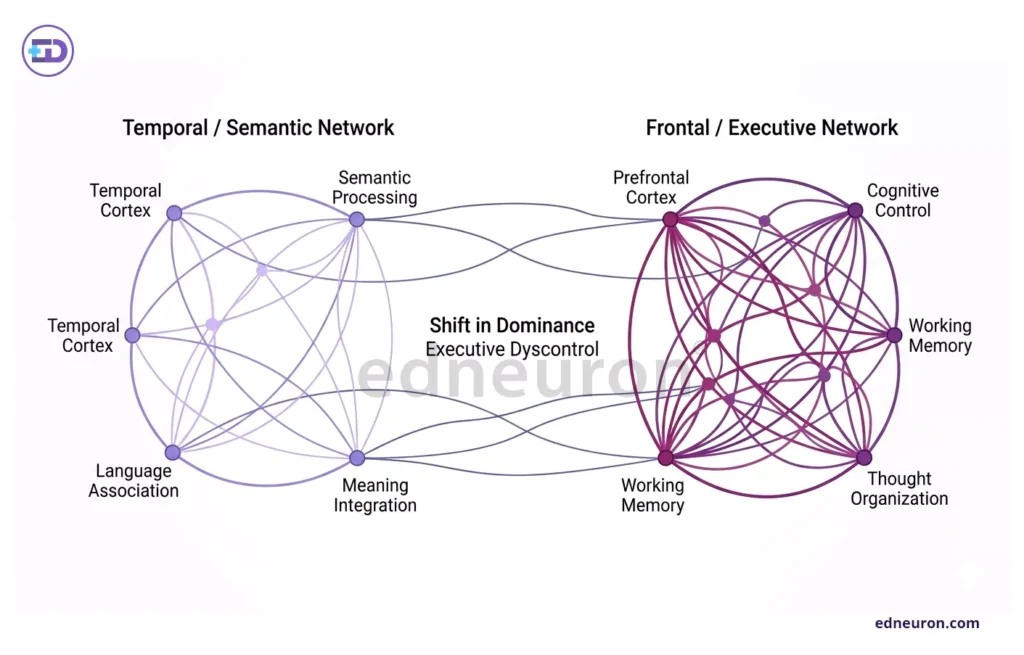
Fig 1: Network illustration highlighting the shift from temporal semantic dysfunction to dominant frontal dysexecutive disruption in formal thought disorder.
The Dysexecutive Shift: Beyond the Temporal Lobe
Traditional neuroimaging often points to the superior temporal gyrus (STG) and Wernicke’s area as key areas involved in FTD. However, looking only at these regions does not explain why disorganized thinking is so closely tied to problems with planning and sequencing actions. Recent studies using resting-state functional connectivity (rsFC) show that while temporal regions may make someone more likely to develop FTD, the severity of positive FTD is better predicted by the connectivity between the right middle frontal gyrus (MFG) and the inferior parietal lobule (IPL).
These brain regions are not mainly responsible for language. Instead, they are important for working memory and social thinking. This means that positive FTD is less about trouble finding the right word and more about problems with the executive control needed to keep thoughts organized. This fits with the idea of “cognitive dysmetria,” in which a faulty thalamic system fails to filter out irrelevant information, leading to the tangential, disorganized speech seen in patients.
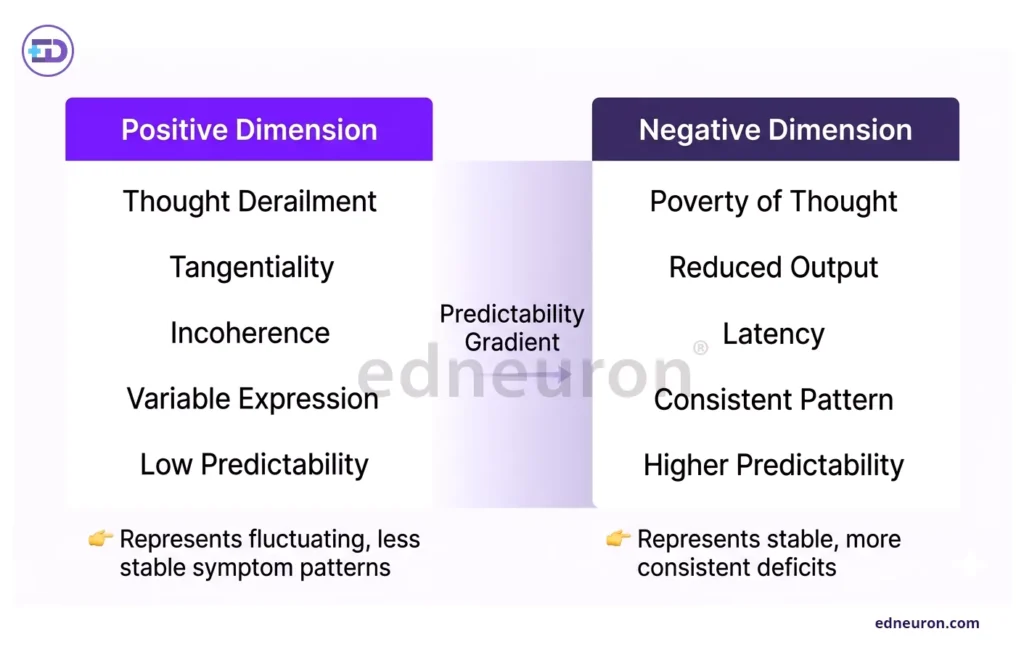
Fig 2: Comparative panels illustrating greater variability and lower predictability in positive thought disorder versus stable, predictable negative dimensions.
The Predictability Gap: Positive vs. Negative Dimensions
There is a clear clinical challenge in that negative FTD, such as poverty of speech, is much harder to detect in the brain than positive FTD. While predictive models can reliably measure the severity of positive FTD, they often cannot do the same for negative FTD. This difference suggests that positive and negative FTD are not merely two ends of a single spectrum but are controlled by distinct brain networks.
Positive FTD seems to be a “noisy” problem in how the brain integrates information, which can be measured as changes in the synchronization of brain activity. In contrast, negative FTD may be a more hidden and lasting problem that is a better predictor of developing schizophrenia in people at high risk. This means that our current brain connectivity models are good at finding disorganized thinking (the “noise”) but not as good at detecting the “silence” of reduced thought.
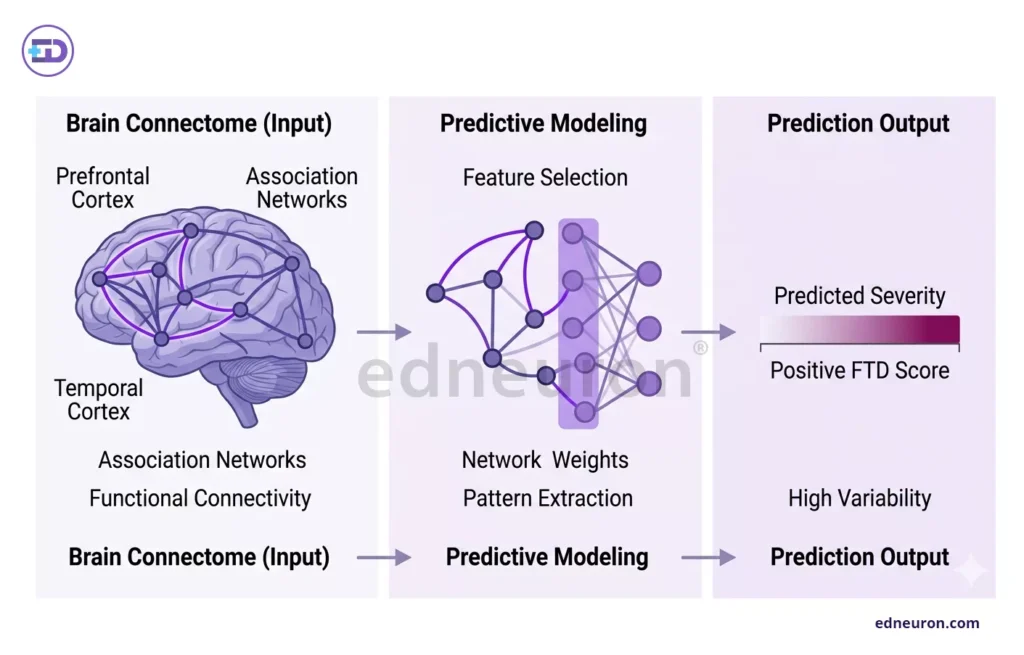
Fig 3: Connectome-based modeling links frontal–temporal connectivity patterns to predicted severity of positive formal thought disorder.
Clinical Outcomes and Real-World Implications
To use these brain connectivity findings in practice, we need to change how we understand patient speech. If positive FTD is mainly a problem with executive function, then treatments that improve executive control and working memory could be just as important as antipsychotic medication. Also, since symptom severity does not match the medication dose, FTD may be a stable brain trait rather than a temporary treatment effect.
Patients can vary a lot. For example, bizarre answers on proverb tests are highly specific (86.89%) for schizophrenia spectrum disorders, even if they are not very sensitive. This means that not all patients with schizophrenia will show clear FTD, but when it is present, it strongly indicates a major change in the person’s ability to use shared understanding to organize their thoughts.
Conclusion
The data show that we should stop seeing “word salad” as a single problem and instead view it as a result of issues in brain networks. Positive formal thought disorder is a measurable failure in the brain’s executive system, caused by problems in how the temporal and frontal areas work together. Understanding FTD as a network problem, not just a language issue, is the first step to using brain imaging in clinical care.
References
- Chen X, Wang Y, Li M, et al. Neurobiological substrates of the positive formal thought disorder in schizophrenia revealed by connectome-based predictive modeling. Neuroimage Clin. 2021;30:102646.
- Kircher T, Krug A, Stratmann M, et al. Differences in single positive formal thought disorder symptoms between schizophrenia and mania. Eur Arch Psychiatry Clin Neurosci. 2021;271(5):847–857.
- Zhang T, Li H, Woodberry KA, et al. Isolated hallucinations are less predictive than thought disorder in psychosis: a longitudinal study. Sci Rep. 2018;8(1):13737.
- Çokal D, Sevilla G, Jones WS, et al. Speech pausing patterns in schizophrenia with and without formal thought disorder: a computational approach. PLoS One. 2019;14(6):e0218727.
- Just SA, Goudbeek MB, et al. Modeling incoherent discourse in non-affective psychosis using computational linguistics. Front Psychiatry. 2020;11:846.
- (Molecular Psychiatry Study Group). Transdiagnostic types of formal thought disorder and their association with gray matter structure. Mol Psychiatry. 2022;27(5):2315–2324.
- Oliva F, Sideli L, et al. Thought and perception disorders in borderline personality disorder compared with schizophrenia. BMC Psychiatry. 2014;14:239.
- Zakowicz K, Białecka-Pikul M, et al. Detection of formal thought disorder in child and adolescent psychosis using machine learning approaches. Front Psychiatry. 2025;16:XXXXX.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



