

Introduction
Psychiatry still relies on a system of distinct diagnoses, with almost 300 listed in the DSM-5, each defined by specific symptoms and their timing. However, as precision medicine advances, a clear clinical conflict has emerged: the categories we use to treat patients do not align with the complex neurobiological and genetic nature of these conditions. Bipolar disorder (BD) is a prime example, connecting psychosis and mood disorders, and its molecular structure points to a problem with the brain’s ability to regulate itself rather than clear-cut categories.
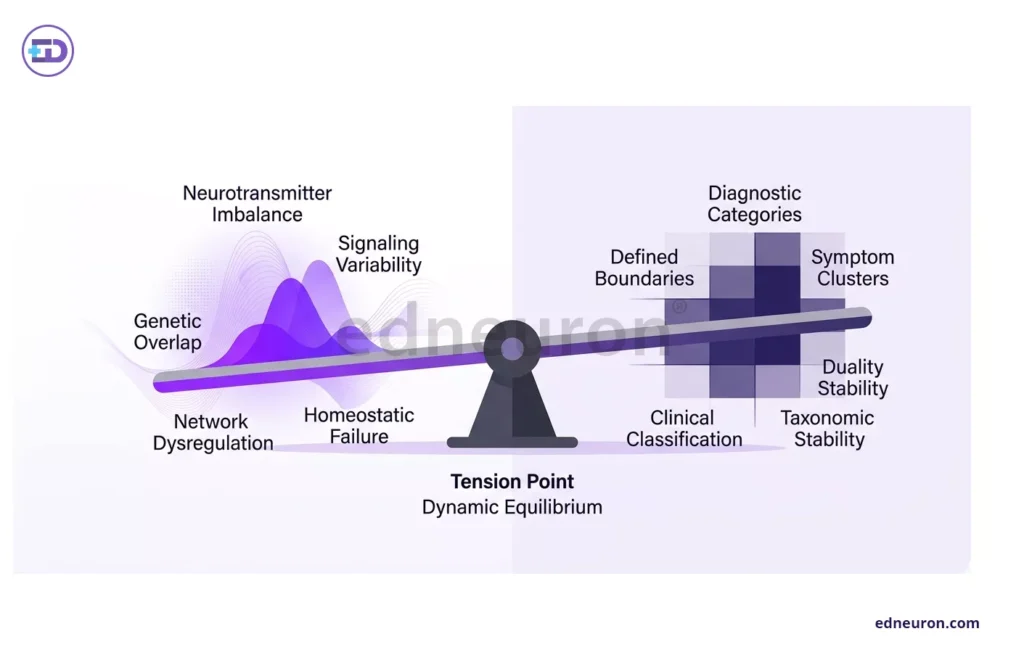
Fig 1: Seesaw schematic illustrating the tension between dynamic molecular dysregulation and stable categorical diagnostic frameworks.
The Molecular Seesaw: Homeostatic Failure vs. Categorical Stability
The dopamine hypothesis of BD helps explain why the illness cycles between different states. Research shows that mania is linked to high dopamine levels, especially increased D2/3 receptor activity, while depression may be caused by a rise in dopamine transporter (DAT) levels, which lowers dopamine function. This means BD is not simply a permanent chemical imbalance, but rather a problem with the brain’s ability to maintain stability.
Despite this clear mechanism, real-world treatment is more complex. We use D2 blockers to treat mania caused by high dopamine, but these drugs also help with bipolar depression, which is puzzling and not fully explained. It may involve other pathways, such as serotonin or the AKT/glycogen synthase kinase 3 cascade. This leads to an important question: are our treatments addressing the root cause of the disease, or just controlling symptoms in a system that is out of balance?
The Genetic Overlap and the Cost of Rigid Boundaries
Modern genetics challenges our traditional way of classifying mental illnesses. Large genome-wide association studies (GWAS) show strong genetic links between BD, schizophrenia (SCZ), and major depressive disorder (MDD). BD I shares more genetic risk with schizophrenia than BD II does. This means that genetic risk for psychiatric symptoms spans diagnostic categories, supporting a dimensional model rather than strict categories.
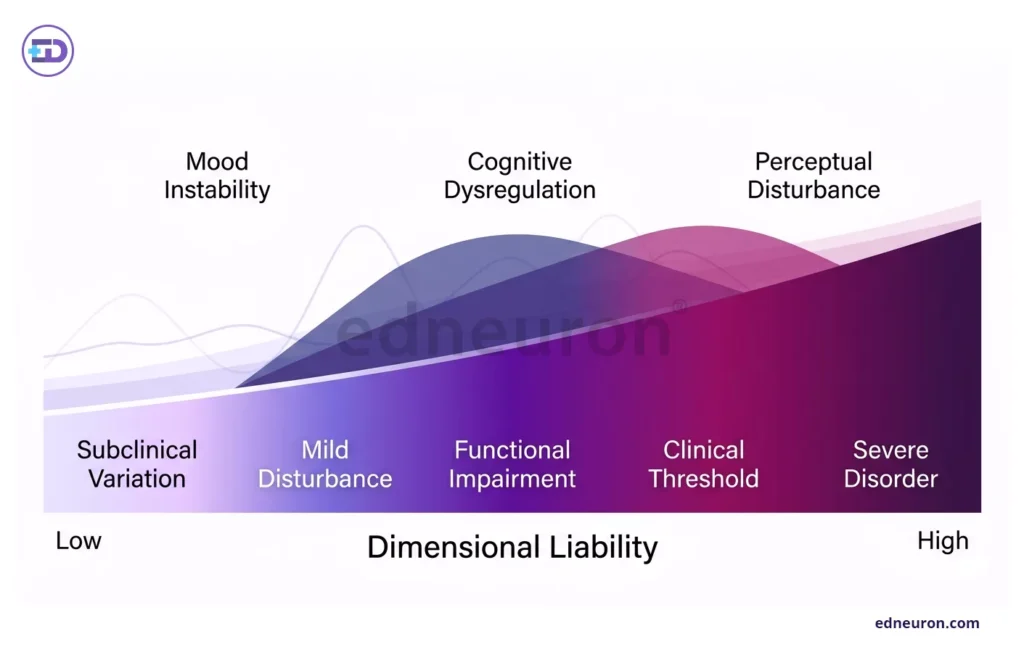
Fig 2: Continuous liability spectrum illustrating graded progression from subclinical variation to severe psychiatric disturbance across overlapping domains.
The effects of these blurred boundaries are clear when treating psychosis. If a young adult quickly worsens mentally, we often diagnose “first-episode psychosis” and start antipsychotics. However, sometimes the symptoms are caused by a neurological problem, like anti-NMDA receptor encephalitis. In these situations, a wrong diagnosis can be very harmful; antipsychotics might hide the real issue, while the underlying neurological problem goes untreated, which can lead to preventable illness or death.
Clinical Outcomes and the Burden of Imprecision
Focusing only on symptoms can make us overlook the physical health of people with bipolar disorder. These patients are much more likely to have obesity, diabetes, and heart disease, which often go untreated because psychiatrists are usually their only doctors. Mood stabilizers and atypical antipsychotics are needed for mental stability, but they also bring extra risks, such as causing diabetes and QTc prolongation.
The “paradox of recovery” shows that our treatments can sometimes cause problems similar to the disease itself. For example, a patient whose main symptoms are managed but who becomes apathetic and inactive may not be getting worse, but instead may be experiencing side effects from antipsychotics, such as Parkinsonism or negative symptoms caused by low dopamine in certain brain areas. Clinicians should consider whether a patient’s lack of response is due to the illness or to treatment effects.
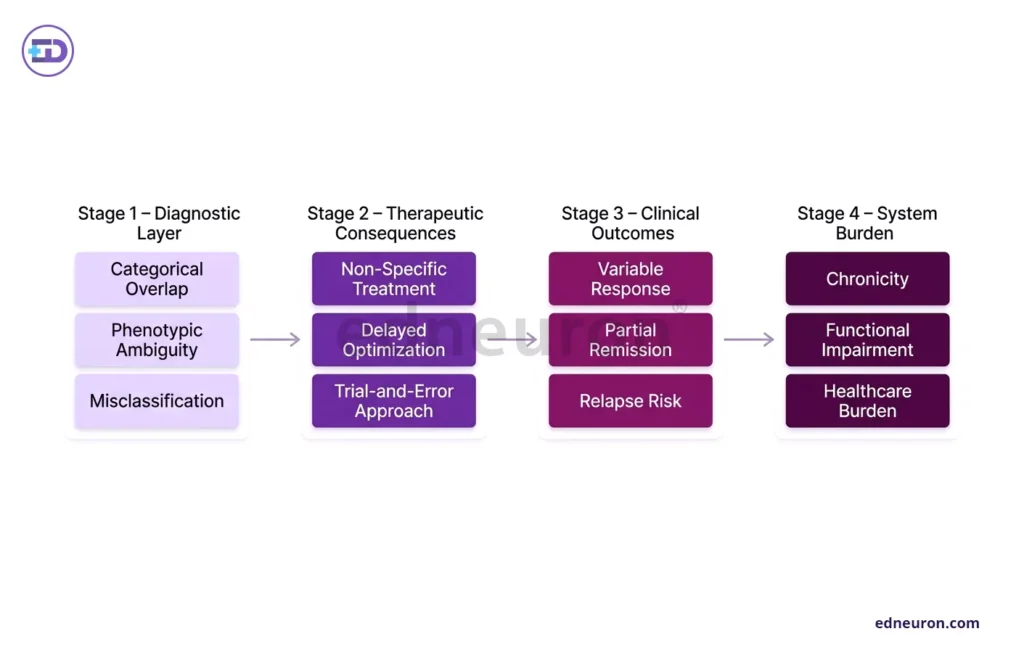
Fig 3: Diagnostic imprecision cascades from misclassification to suboptimal treatment and ultimately worsened clinical and system-level outcomes.
Conclusion
There is no simple solution, but this situation calls for clinical humility. Our current classification system is useful for communication, but it does not reflect the true nature of these disorders. To improve, we need to incorporate genetics and the physical basis of disease into a “neurocircuit-based taxonomy” that focuses on specific network problems, such as emotional overreaction or movement issues, rather than relying on labels. Success comes from understanding that while the DSM gives us names, it is the patient’s genetics and brain circuits that shape their condition.
References
- Charney AW, Ruderfer DM, Stahl EA, Moran JL, Chambert K, Belliveau RA, et al. On the diagnostic and neurobiological origins of bipolar disorder. Transl Psychiatry. 2020;10(1):156.
- Bi B, Xiao Y, Wu C, Cao L, Fang Y, Zhang Y, et al. Neural network of bipolar disorder: Toward integration of neuroimaging and neurocircuit-based treatment strategies. Transl Psychiatry. 2022;12(1):97.
- Ashok AH, Marques TR, Jauhar S, Nour MM, Goodwin GM, Young AH, et al. The dopamine hypothesis of bipolar affective disorder: The state of the art and implications for treatment. Mol Psychiatry. 2017;22(5):666–79.
- McLaren KD, Marangell LB. Special considerations in the treatment of bipolar disorder with medical comorbidities. Ann Gen Psychiatry. 2004;3:7.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



