
Introduction
In acute psychiatric care, when patients show ‘bizarre’ behaviors, disorganized thinking, and severe suicidality, clinicians often quickly diagnose first-episode psychosis (FEP). While this approach helps start antipsychotic treatment, it can also overlook severe obsessive-compulsive disorder (OCD), especially when obsessions have become fixed beliefs. The main clinical challenge is not just identifying symptoms, but understanding where they come from: is this a true break from reality, or the result of a patient worn down by untreated obsessive thoughts?
Fig 1: A depiction of severe OCD with absent insight, where structured compulsions are misperceived as psychosis through a distorting diagnostic veil.
Case Presentation
A 31-year-old woman with a history of high functioning was brought to the emergency department after she was found holding a knife to her wrist. This happened after a month of increasing anxiety, restlessness, and a serious drop in her ability to function. At first, doctors noticed ‘bizarre’ behaviors, such as chewing through bedsheets and shirts and biting her own cheek, as well as a flat affect, poor eye contact, and disorganized speech.
The patient said her brain felt ‘fried’ and was convinced that she and her husband would ‘go broke’ and ‘die penniless,’ even though there was no evidence for this. In the emergency room, her disorganized thinking and unpredictable safety behaviors led doctors to suspect first-episode psychosis. Later, more detailed interviews showed she had a 15-year history of symmetry fixations and counting compulsions that had never been diagnosed. Her Yale-Brown Obsessive Compulsive Scale (YBOCS) score was 38 out of 40, showing extreme severity, and her Brown Assessment of Beliefs Scale (BABS) score of 21 showed she had no insight and held delusional beliefs.
Clinical Analysis: The Insight Spectrum and Phenomenological Overlap
This case stands out because the severity of the patient’s obsessions made them hard to recognize. In the past, OCD was thought to always involve ‘good insight,’ but now we know that insight can range from good to absent. When a patient lacks insight, it can be difficult to distinguish between an ‘obsession’ and a ‘delusion,’ since the patient is completely convinced of their thoughts.
The patient’s ‘bizarre’ behaviors, like chewing through sheets and wringing her hands, were not signs of psychosis but desperate attempts to feel in control during intense inner stress. This shows how easily OCD can be missed; about 70% of people who meet OCD criteria are never formally diagnosed, often because doctors focus on more obvious symptoms of psychosis or mood disorders. In this case, her suicidal thoughts were not a main symptom but a reaction to her belief that financial and health disaster was unavoidable.
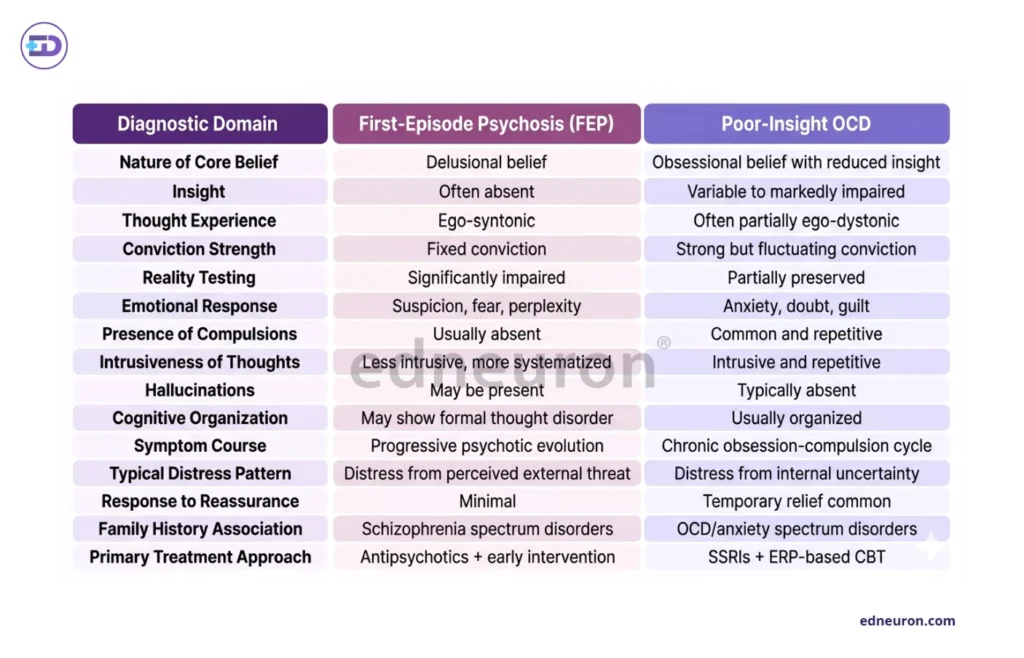
Table 1: Comparative clinical features distinguishing first-episode psychosis from poor-insight obsessive-compulsive disorder.
Treating these ‘schizo-obsessive’ cases needs careful medication choices. This patient improved with high-dose sertraline and aripiprazole, but research shows that second-generation antipsychotics (SGAs) should be used to support, not replace, other treatments in these situations. In her case, using buspirone earlier may have actually made her anxiety even worse.
Clinical Implications
This case clearly shows that losing the ability to function is not unique to schizophrenia. A person can go from being highly capable to being unable to drive or cook because of severe OCD alone. For specialists, the main lesson is to be patient and look closely at the patient’s experience. If the doctor had only focused on the first ER signs, like ‘knife to wrist’ and ‘chewing sheets,’ the patient might have been treated for psychosis with high-dose antipsychotics for life, even though she did not have a primary psychotic disorder.
Instead, discovering her long-standing symmetry fixations changed the treatment focus from stopping hallucinations to helping her learn to resist compulsions and change her thinking patterns.
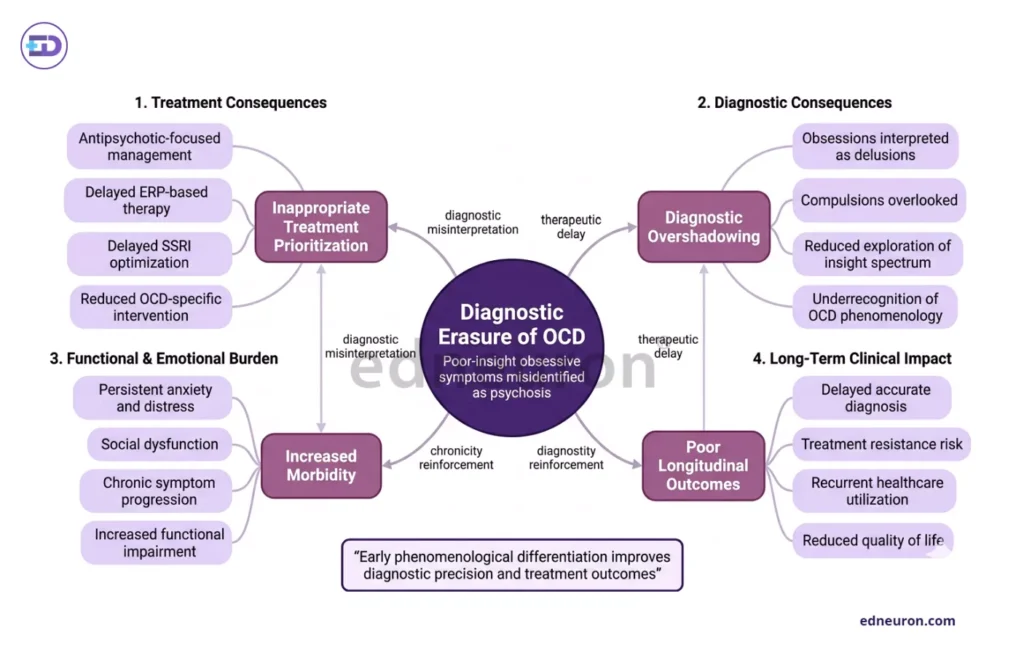
Fig 2 : Clinical consequences arising from misidentification of poor-insight OCD as primary psychotic illness.
Conclusion
The diagnostic boundary between psychosis and severe OCD is not a line, but a territory of significant overlap. When “delusions” are rooted in an obsessive-compulsive history, the standard FEP pathway may fail. True recovery for these complex patients requires a clinician who pauses to ask whether the “psychotic” behavior is, in fact, the final, desperate ritual of a mind trying to regain a sense of control.
References
- Sharma A, Gupta R, Verma P. Severe harm-related obsessive-compulsive disorder with violent compulsions: a case report. Psychiatry Res Case Rep. 2026;5(1):100123.
- Khan M, Ali S, Rahman A, et al. Obsessive-compulsive disorder associated with temporal lobe porencephaly: a case report. BMC Psychiatry. 2025;25:112.
- Patel V, Singh H, Choudhury S. Obsessive-compulsive disorder presenting as first-episode psychosis with suicidal ideation: a case report. Cureus. 2023;15(7):e41234.
- Reddy YCJ, Rao NP, Khanna S. Episodic obsessive-compulsive disorder with complete inter-episode remission: a case report. Indian J Psychiatry. 2010;52(2):185–187.
- El-Hage W, Fakra E, Azorin JM. Obsessive-compulsive disorder presenting as dysphagia: a case report. Middle East Curr Psychiatry. 2020;27:77.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



