

Abstract
Systemic lupus erythematosus (SLE) has long been seen as a disease of chronic immune dysregulation requiring indefinite pharmacologic suppression. The rise of the CD19-targeted chimeric antigen receptor T-cell (CAR-T) therapy, which produces deep serologic remission, complement normalization, and drug-free disease quiescence in patients who were failed by conventional immunosuppression, compels a reimagination of lupus in the realm of autoimmune diseases. This article focuses on tenets of the understanding of refractory SLE, shifting from viewing it as a disease of ongoing, perpetual inflammation to a self-reinforcing, maladaptive immune-memory state encoded within autoreactive B-cell lineages, memory clones, plasma-cell precursors, and mutually reinforcing T–B-cell interaction loops. What CD19 CAR-T cells do is transiently erase the immunologic memory of autoimmune identity, thereby permitting de novo reconstitution of a less autoreactive immune repertoire, unlike corticosteroids, which suppress the immune system. We view and contend in depth about limitations of rituximab, belimumab, cyclophosphamide, and conventional immunosuppression, analyzing the kind of B-cell reconstitution that takes shape after CAR-T depletion and discussing the substantial uncertainties that remain, including relapse, infection risk due to hypogammaglobulinemia, economic inequity, and whether remission after CAR-T reflects tolerance restoration to autoantigens or prolonged compartmental depletion.
The Inadequacy of the Suppression Disease Model
Lupus has been managed for the better part of six decades either through modalities that deplete the B cell population or prevent BAFF-dependent B cell survival. Traditional therapies include
- Corticosteroids, which blunt cytokine cascades
- Mycophenolate mofetil and cyclophosphamide, which impair autoreactive B cell expansion/lymphocyte proliferation
- Belimumab (a monoclonal antibody) reduces BAFF activity, and rituximab depletes circulating CD20-positive B cells.
These therapies, built on suppression theory, aim to manage autoimmune disease. Each of these interventions inhibits a component alleged to cause the downstream consequences of chronic inflammation and partially achieves that, but none reliably produces flare-free remission after withdrawal. When we see an archetypal lupus patient requiring indefinite maintenance therapy, punctuated by flares that demand escalation of long-term toxic drugs, accumulating organ damage, and a cycle of drug treatment with no period of sustained relief, it brings no surprise that clinical reality is where conventional therapies are managing lupus activity without addressing its root cause. The question is whether that cause is accessible to therapeutic intervention or, in some meaningful sense, is constitutive of the immune system as it has been rewritten by years of autoimmune experience. CD19 CAR-T therapy now offers a biological challenge to this assumption, and the preliminary answer is more provocative than the field had anticipated.
Lupus as a Disease of Pathologic Immune Memory
We now have evidence that Lupus does not stem solely from persistent inflammation but is deeply ingrained with a self-sabotaging memory, resembling a self-reinforcing network in which autoreactive B cells receive help from follicular helper T cells already primed by autoantigenic peptide presentation. Long-lived plasma cells can independently produce autoantibodies via TLR7 signaling, thereby spontaneously generating germinal centers that refine autoantibody affinity through somatic hypermutation and class switching. Immune complexes deposit in tissue, driving complement consumption and generating new antigen that feeds the cycle through epitope spreading. Toll-like receptors, especially TLR7/9, activate autoreactive lymphocytes at subthreshold stimuli, promote plasmablast differentiation, and maintain a persistent innate immune tone that refreshes the adaptive autoimmune response. The result is not inflammation that burns and resolves, or an open-and-shut case,, but a closed circuit continuously replenishing the faulty constitution using its own encoded experience as the template. One might think that if the disease is maintained by encoded memory rather than by acute inflammation, then suppressing the inflammatory output while preserving the memory cannot surely produce durable remission. What is required is access to the memory itself, and this is precisely what CD19 CAR-T therapy appears to provide, at least provisionally.
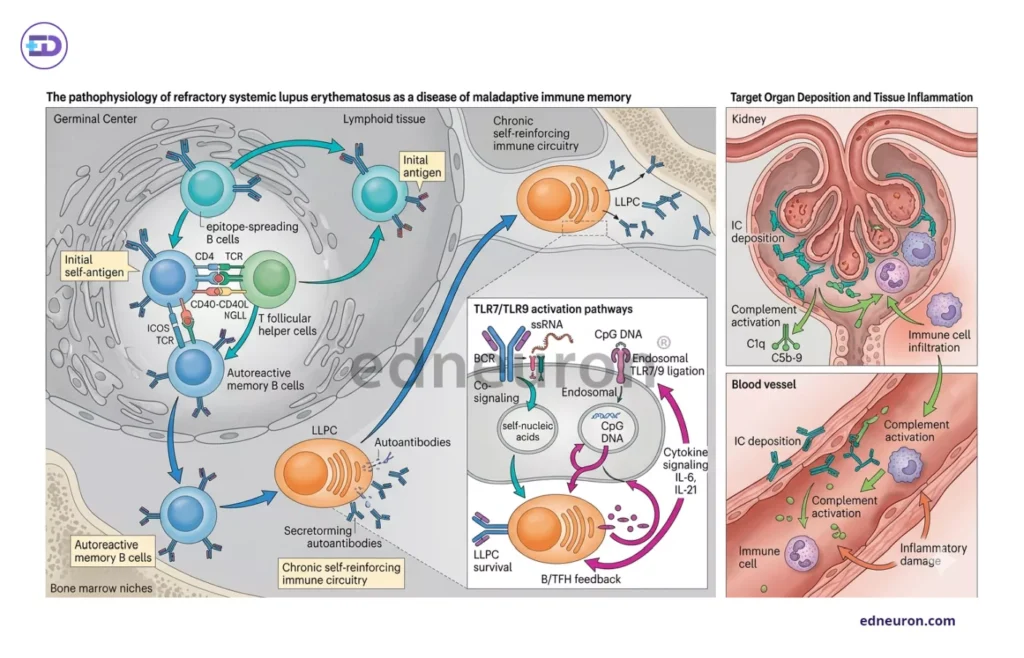
Fig 1 : Pathophysiology of SLE as a disease of maladaptive Immune memory rather than persistent chronic inflammation.
Why Rituximab and Belimumab provided an incomplete solution
Rituximab is a CD20-directed monoclonal antibody that depletes mature B cells by antibody-dependent cell-mediated cytotoxicity/cellular phagocytosis, thereby removing autoantibodies and treating the disease. The clinical experience has been substantially more complicated; for example, the EXPLORER study found no difference in benefit between the Rituximab and placebo groups among patients with severe extrarenal SLE. Rituximab incompletely depletes B-cell compartments, particularly at tissue sites, including plasmablasts and long-lived plasma-cell populations that do not express CD20. Studies find that, by virtue of the autoimmune niche, some B cells become refractory to attempts at depleting them, and autoreactive memory B cells negative for CD20 persist, protected within lymphoid and ectopic lymphoid structures. Tertiary lymphoid organizations that emerge within inflamed lupus kidneys and synovium sustain the local autoantibody production independent of circulating depletion.
Belimumab, another newer drug for severe SLE, blocks BAFF (B-cell activating factor) and is an indispensable trophic survival signal for naive and transitional B cells. Post-treatment, in either therapy, anti-dsDNA titers fall and complement proteins normalize, but the effects are transient. Patients show recovery, with plasmablasts number and surviving memory clones proliferating to repopulate the depleted compartment. The problem is that it does not erase memory; it only modifies the survival of new B cells, without deleting the code responsible for disease experience. Moreover, some B cells that already underwent affinity maturation over years of germinal center activity are not particularly sensitive to BAFF withdrawal, as their survival depends more on memory-maintenance signals than BAFF-driven trophic.
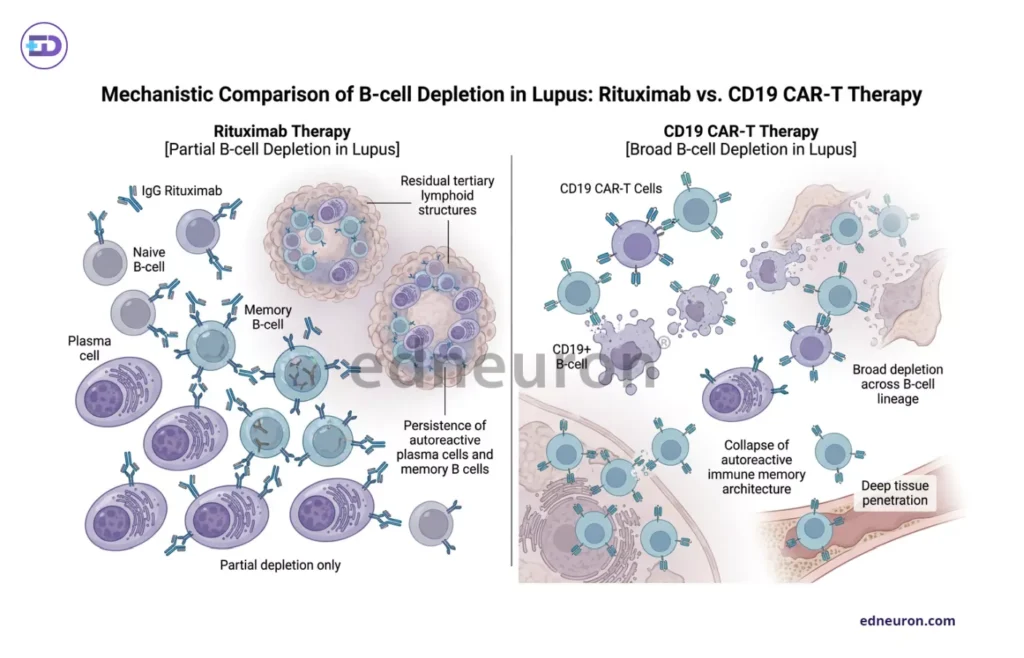
Fig 2 : Comparative panel of B-cell depletion via Rituximab vs CD19 CAR-T therapy.
CD19 CAR-T and the Biology of Immune Reset
CAR-T is an innovation that originated in hopes of finding a treatment for B-cell lymphoma. The scientists take autologous T cells, which are genetically engineered with receptors whose extracellular domain targets CD19 on B cells while the intracellular domain contains co-stimulatory and IL-2Rβ (gen V) domain to enhance T cell in vivo expansion and survival. The serologic findings when treating a patient with refractory SLE are not merely a quantitative reduction in autoantibody titers, but antibodies that had persisted for years despite cyclophosphamide and rituximab become undetectable. More striking is when B cells reconstituted emerging from a CD19-depleted nadir weeks after infusion, the repopulating compartment consists predominantly of naïve B cells, immunologically inexperienced, without the autoreactive repertoire characteristics that had defined the pre-treatment immune landscape. This is distinct from what rituximab achieves. CD19 CAR-T cells target a broader spectrum of B-cell lineages, including plasmablasts and plasma-cell precursors, which would otherwise escape CD20-targeted depletion. The fact that these engineered cells can infiltrate tissue compartments, accessing autoreactive reservoirs in tertiary lymphoid structures and inflamed organs that otherwise elude the circulating antibodies, makes them better positioned to achieve better clinical outcomes. The newer BCMA compound CAR-T approach clears CD19-negative BCMA-positive bone marrow residents that were previously insulated, destroying the final reservoir of autoantibodies. Patients with grade III/IV lupus nephritis, dual targeting produced complement recovery, proteinuria resolution, and drug-free remission of greater durability than CD19 depletion alone.
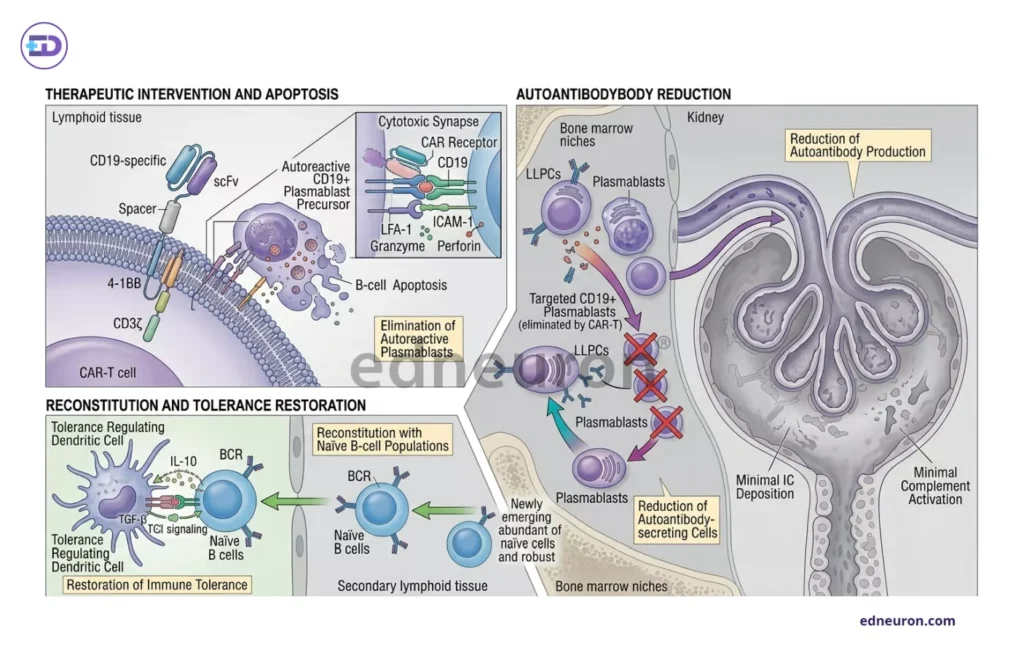
Fig 2 : Mechanism of CART cells.
The Operational Cure Question
The concept of operational cure, as defined in oncology, is not the biological impossibility of disease recurrence but rather a state of prolonged, treatment-free disease withdrawal indistinguishable from normality; it has rarely been applied to systemic autoimmunity. Lupus, in particular, has been considered a lifelong condition requiring chronic pharmacologic management. The early CAR-T data challenge this assumption with a directness that demands serious engagement.
Several observations support the possibility that CAR-T is doing something more than producing prolonged depletion. When we simultaneously analyze autologous stem cell transplantation, in which myeloablation followed by immune reconstitution produces long-term drug-free remission in refractory SLE, decades before CAR-T was clinically available, a more astute question arises- whether this suggests tolerance, in which self-reactive lymphocytes are deleted, rendered anergic, or suppressed by regulatory mechanisms, or merely to a prolonged ghosting of the cellular infrastructure needed to regenerate autoreactive responses, and is worthy of deliberation. The two may seem synonymous, but are not: tolerance implies that the reconstituting immune system has been re-educated to recognize and ignore the autoantigens that previously drove disease. Depletion implies only that the autoreactive clones are absent and may return, given sufficient time and immunologic provocation. The data from existing cohorts do not yet resolve this question, and longer follow-up periods in larger patient populations are necessary before treatment with CAR-T can be confidently classified as an achievable cure for SLE.
Limitations, Risks, and the Boundaries
- Short-term side effects: Cytokine release syndrome (CRS), which is rarer in its occurrence in autoimmune patients, is a procedural risk requiring institutional expertise. Immune effector cell-associated neurotoxicity syndrome (ICANS) has been observed in a minority of patients, and the neurologic risk profile in younger lupus patients, many of whom have neuropsychiatric SLE, requires careful longitudinal monitoring.
- The long-term hematologic consequences of sustained B-cell aplasia, particularly hypogammaglobulinemia, carry an infection risk that is not trivial in a patient population already immunocompromised by disease and prior therapy. Whether long-term immunoglobulin replacement will be required in a meaningful proportion of patients who achieve durable remission is unknown. The question of relapse- when and why some patients experience autoreactive B-cell populations while others do not- remains unresolved and clinically crucial.
- Finally, the money/logistical requirements, unavailability of resources in low-income settings, and the lengthy manufacturing process for CART cells do not allow for a global solution until scalable manufacturing via allogeneic, off-the-shelf, or in vivo CAR platforms is achieved.
Conclusion
If refractory lupus can enter a state of drug-free remission following engineered deletion of its B-cell memory, and if the recuperating immune system fails to recapitulate the same autoreactive repertoire that caused the disease, then lupus cannot simply be a disease of dysregulated immunity but one of corrupted immune identity, etched within cellular lineage and maintainable only as long as the encryption is translated and is carried forward. This, in itself, is prima facie evidence that the boundary between immune suppression and immune cure is not fixed by an absolute law but by the depth to which an intervention engages the memory substrate. CAR-T therapy may offer, for the first time, access to a temporary but complete erasure of the autoreactive memory state. Whether this constitutes a cure, a prolonged remission, or a deferred recurrence will be determined by springs of science not yet discovered or fully understood.
References
- Müller F, Taubmann J, Bucci L et al. CD19 CAR T-Cell Therapy in Autoimmune Disease – A Case Series with Follow-up. N Engl J Med. 2024 Feb 22;390(8):687-700. PMID: 38381673.
- Merrill JT, Neuwelt CM, Wallace DJ et al. Efficacy and safety of rituximab in moderately-to-severely active systemic lupus erythematosus: the randomized, double-blind, phase II/III systemic lupus erythematosus evaluation of rituximab trial. Arthritis Rheum. 2010 Jan;62(1):222-33. PMID: 20039413.
- Navarra SV, Guzmán RM, Gallacher AE et al. BLISS-52 Study Group. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: a randomized, placebo-controlled, phase 3 trial. Lancet. 2011 Feb 26;377(9767):721-31. PMID: 21296403.
- Zhou J, Lei B, Shi F et al. CAR T-cell therapy for systemic lupus erythematosus: current status and future perspectives. Front Immunol. 2024 Dec 19;15:1476859. PMID: 39749335.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi


