

Abstract
Tracheostomy insertion is stringently regulated by a myriad of validated indications, procedural protocols, and a broadly accepted timing criterion. Contrarily, tracheostomy removal is not. Even with advancements spanning four decades in the fields of ICU liberation, respiratory physiology, swallowing assessment, and airway management, the essential decision of the timing of decannulation still persists as one of the least standardized consequential decisions in acute and post-acute medicine. The inability of any one physiologic threshold- the successful reintegration of airway patency, swallow competence, cough mechanics, secretion clearance, or a neurologic recovery into a self-sustaining respiratory system- to anticipate decannulation with favorable outcomes shows a deeper systems problem that removal assesses. This commentary argues that decannulation must be reconceptualized as a multisystem rehabilitation endpoint that is physiology-guided rather than practice.
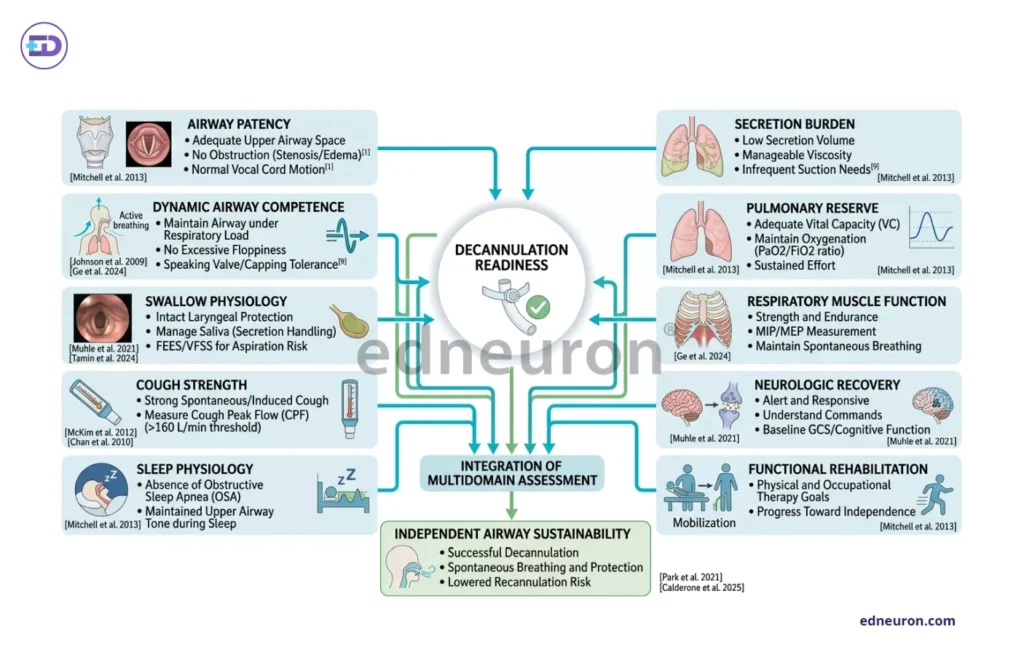
Fig 1 : Multidomain Physiologic Framework for Tracheostomy Decannulation Readiness.
Airway Patency is Not Airway Competence
The assumption that an anatomically unobstructed airway is a decannulatable airway remains one of the most critical conflation and probably half-baked presumptions in care medicine. Patency (the passive absence of fixed obstruction) and competence (the dynamic capacity to protect the airway under physiologic stress) are distinct. Tracheostomy tube manometry studies demonstrate that downsizing reduces airway resistance and increases capping feasibility, but resistance measured through a capped tube approximates and does not aid in realizing the work-of-breathing burden a patient will sustain after decannulation. What these capping trials and an endoscopic assessment do is help establish upper-airway continuity and evaluate resistance, but they fail to support the demand/ability to breathe independently without an indwelling tube.
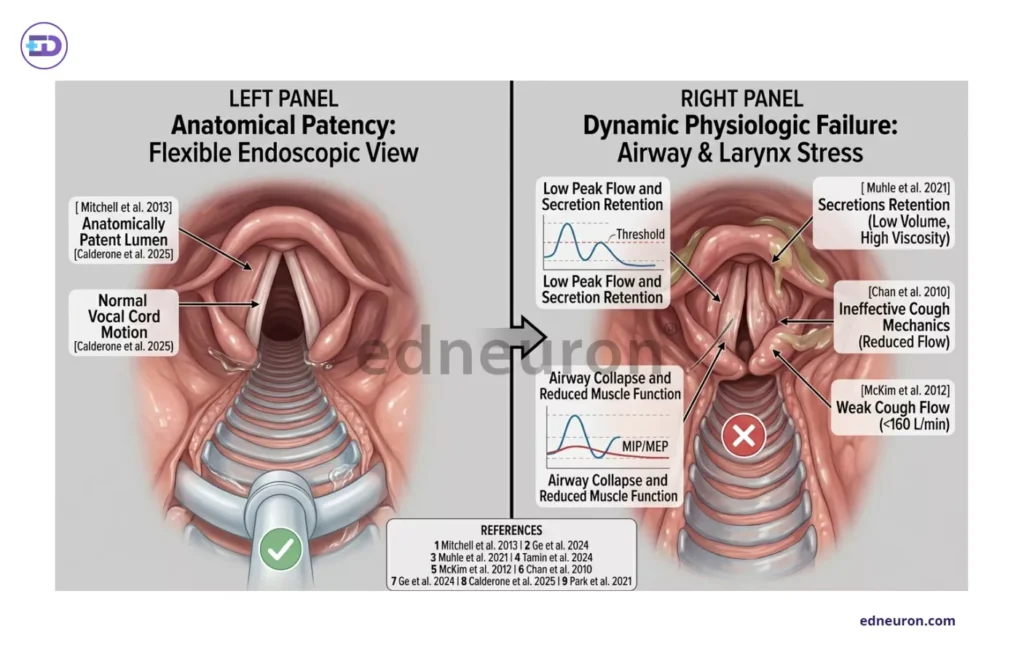
Fig 2 : Airway Patency Does Not Equate to Functional Airway Competence.
Swallowing Physiology is Necessary but Not Sufficient
The integration of fibreoptic endoscopic evaluation of swallowing (FEES) and videofluoroscopic swallow study into decannulation pathways represents a genuine advance with a genuine risk of diagnostic overreach. The SESETD protocol helps elucidate that structured assessment of secretion management, spontaneous swallowing frequency, and laryngeal sensory integrity can be performed reproducibly. The difficulty is interpretive for a patient who passes a swallow evaluation and still fails decannulation, either because of inadequate cough, excessive secretion burden, or respiratory muscle insufficiency, something which slips right underneath the assessment’s detection. In patients, especially with post-intubation laryngopharyngeal sensory dysfunction, silent aspiration can persist despite clinically acceptable swallowing and neurogenic dysphagia following GBS. We see and do realize that swallowing physiology is a necessary domain of decannulation assessment. It is not, and cannot be, a sufficient one.
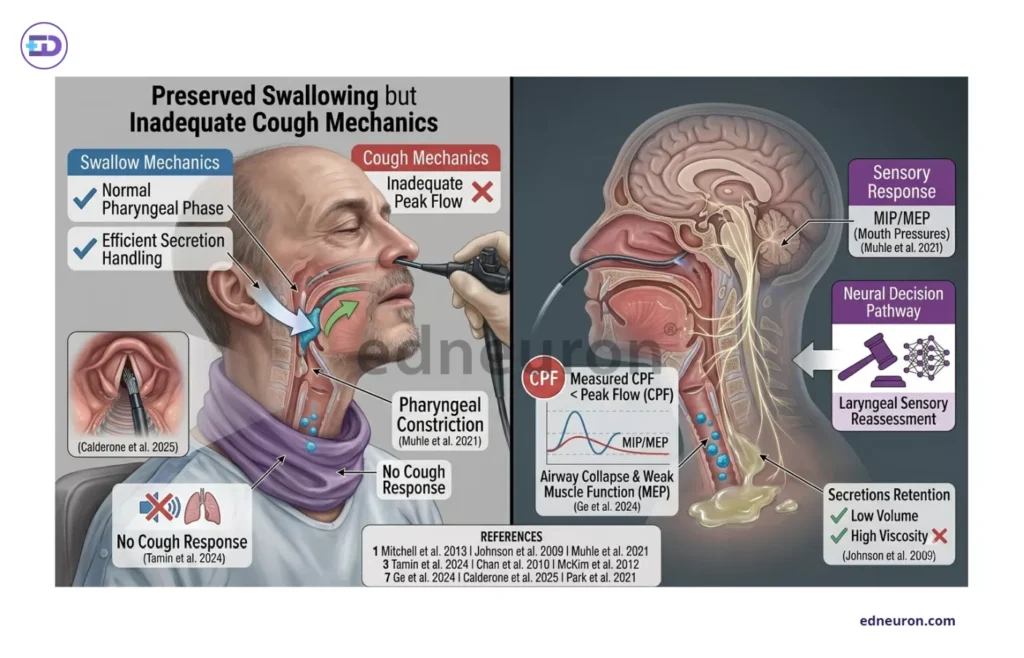
Fig 3 : Preserved Swallowing Function Does Not Necessarily Predict Decannulation Success.
The Overlooked Problem of Overburdening Secretions in Decannulation
Decannulation failure is more frequently attributed to secretion failure rather than airway failure. Peak cough flow, which is measurable by a capped tube or a speaking valve, is considered to be the most physiologically grounded predictor of decannulation success, with threshold variation being reported between 29 L/min and 100 L/min, based on the measurement technique and patient population. The context of measurement matters as much as the threshold itself. Capped tube-assisted cough, which is consistently associated with higher flows than spontaneous cough after tube removal, thereby biasing the pre-decannulation assessment toward optimism. We find that, as corroborated by Calderone and the fellow researchers in a scoping review published in 2025, parameters such as strong respiratory function, effective secretion management, and elevated GCS scoring and low BMI values are some of the most reliable and strong predictors of successful decannulation across varied populations analyzed, including patients with stroke, pediatric cohorts, and elderly patients with adverse effects and severe comorbidities. What remains disheartening is that such useful data remain unrealized as long as we have a framework in which the secretion burden scoring remains institutionally inconsistent, mucociliary clearance rarely being formally assessed, and the weakness of respiratory muscles that we so often encounter in ICU survivors and patients with neuromuscular disease, which is frequently inferred rather than measured. The field has debated airway thresholds for decades, while underspecifying the secretion physiology that determines whether those thresholds are clinically meaningful remains unclear.
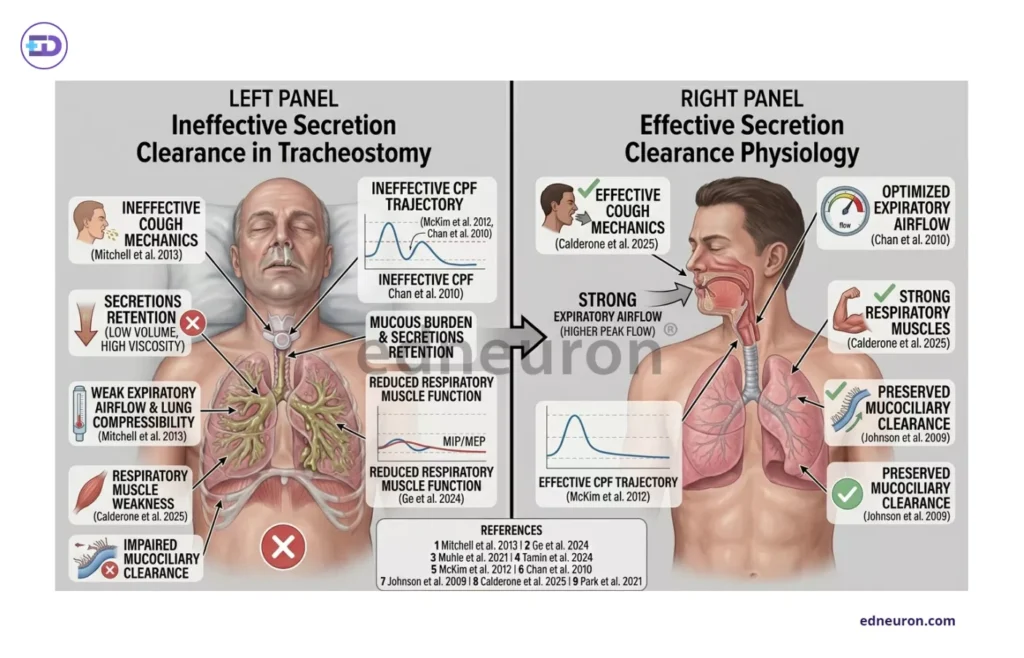
Fig 4 : Determinants of Effective Versus Ineffective Secretion Clearance Physiology in Tracheostomy Decannulation.
A Decision Across Specialties
Tracheostomy decannulation is managed by multiple specialities in various institutions: otolaryngology, pulmonology, critical care medicine, rehabilitation medicine- speech therapy. All of these domains differ markedly in risk tolerances, physiologic priorities, and outcome definitions, and are based on different priorities:
- Otolaryngology emphasizes airway patency and endoscopic confirmation.
- Critical care medicine prioritizes respiratory stability and the management of secretions.
- Rehabilitation medicine favors functional recovery, cognitive status, and long-term rehabilitation potential.
The DECAN predictive model captures this complexity by incorporating age, BMI, malignancy, neurologic disease, vasopressor dependence, delirium, and pneumonia as decannulation predictors. This list cannot be mapped to any single specialty and requires interprofessional quality improvement programs to reduce time to decannulation and adverse events. The pathways vary substantially across institutions, so decannulation readiness remains, in practice, more of a multidisciplinary judgment than a validated diagnostic determination. Medicine standardized the insertion of the tracheostomy tube. It never standardized its removal.
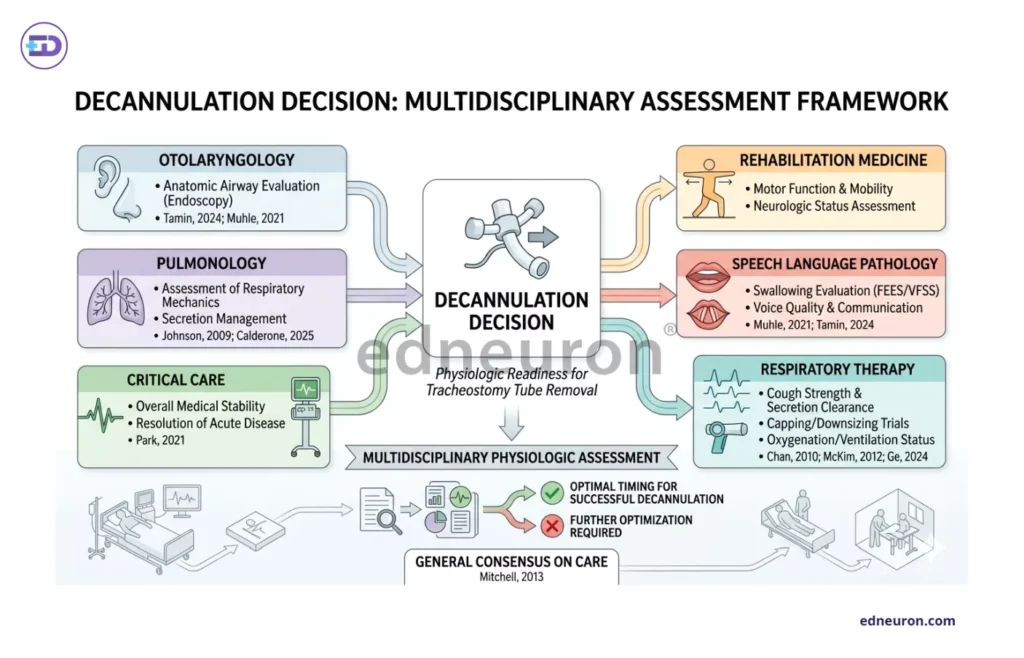
Fig 5 : Multidisciplinary Physiologic Framework Guiding Tracheostomy Decannulation Decision-Making.
Onto the Physiology-Guided Path
Decannulation represents the final test of airway physiology, swallowing, pulmonary reserve, secretion clearance, and neurologic recovery successfully being lignified into a self-sustaining respiratory system. A patient does not become decannulatable because a capping trial is tolerated or a swallow study is passed. They become merit removal only when the convergence of those domains reaches a threshold sufficient to sustain independent airway function across the full range of physiologic demand- during sleep, during secretion load, neurologic fatigue, and during the unremarkable stress of daily existence. Achieving a standardized protocol requires moving from varied institutional checklists to a validated multidomain physiological assessment framework. The evidence base exists in fragments, and it has not yet been formulated clinically. This existing gap reflects the system’s failure rather than clinical curiosity. This procedural gap is one that the field needs to reach consensus on and eliminate with haste.
References
- Mitchell RB, Hussey HM, Setzen G, et al. Clinical consensus statement: tracheostomy care. Otolaryngol Head Neck Surg. 2013 Jan;148(1):6-20. PMID: 22990518.
- Johnson DC, Campbell SL, Rabkin JD. Tracheostomy tube manometry: evaluation of speaking valves, capping, and need for downsizing. Clin Respir J. 2009 Jan;3(1):8-14. PMID: 20298366.
- Muhle P, Suntrup-Krueger S, Burkardt K, et al. Standardized Endoscopic Swallowing Evaluation for Tracheostomy Decannulation in Critically Ill Neurologic Patients – a prospective evaluation. Neurol Res Pract. 2021 May 10;3(1):26. PMID: 33966636.
- Tamin S, Shabrina F, Hutauruk SM, et al. A cross-sectional study comparing standardized evaluation for tacheostomy decannulation to flexible endoscopic evaluation of swallowing examination. Med J Malaysia. 2024 Mar;79(2):119-123. PMID: 38553913.
- Chan LY, Jones AY, Chung RC, Hung KN. Peak flow rate during induced cough: a predictor of successful decannulation of a tracheotomy tube in neurosurgical patients. Am J Crit Care. 2010 May;19(3):278-84. PMID: 19435950.
- McKim DA, Hendin A, LeBlanc C, et al. Tracheostomy decannulation and cough peak flows in patients with neuromuscular weakness. Am J Phys Med Rehabil. 2012 Aug;91(8):666-70. PMID: 22561386.
- Ge J, Niu G, Li Q, et al. Cough flows as a criterion for decannulation of autonomously breathing patients with tracheostomy tubes. Respir Res. 2024 Mar 18;25(1):128. PMID: 38500141.
- Calderone A, Filoni S, De Luca R, et al. Predictive Factors of Successful Decannulation in Tracheostomy Patients: A Scoping Review. J Clin Med. 2025 May 28;14(11):3798. PMID: 40507559.
- Park C, Ko RE, Jung J, Na SJ, Jeon K. Prediction of successful de-cannulation of tracheostomised patients in medical intensive care units. Respir Res. 2021 Apr 28;22(1):131. PMID: 33910566.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi


