


Introduction
the emergence of (DI-AIH) as a recognized entity, alongside the popularisation of immune checkpoint inhibitor (ICI) therapy, has rendered the diagnostic landscape considerably more complex than historical models anticipated.Few clinical scenarios in hepatology demand more rigorous diagnostic reasoning than the surface-level differential—autoimmune hepatitis (AIH) and drug-induced liver injury (DILI). Drug-induced autoimmune hepatitis (DIAIH) is a specific entity that occurs at the blurred intersection of AIH and DILI. Idiopathic AIH demands long-term immunosuppression with attendant morbidity. At the same time, like DILI, DIAIH mandates drug withdrawal and expectant management. Misclassification in either direction exposes patients to unnecessary risk. Yet the biological and phenotypic boundaries between these conditions are genuinely permeable, and.
Mechanistic and Clinical Overlap
AIH reflects a breakdown of central or peripheral immune tolerance to hepatocyte autoantigens, with the presence of autoantibodies such as ANA (antinuclear antibodies) and ASMA (anti-smooth muscle antibodies). At the same time, DILI represents hepatocyte injury triggered by direct toxicity, reactive metabolite formation via the CYP450 enzyme machinery, or idiosyncratic immune activation in response to a xenobiotic. In practice, however, this straightforward concept collapses in DI-AIH, where a drug—most commonly nitrofurantoin, minocycline, statins, dihydralazine, methyldopa, or anti-TNF agents—after undergoing metabolism causes sensitization of immune cells due to the nuclear antigens, which trigger an immune response that is serologically and histologically indistinguishable from idiopathic AIH. Antinuclear antibodies (ANA) and Antismooth muscle antibodies (ASMA) appear in both; elevated IgG is common to both, although modestly elevated; and interface hepatitis with plasma cell infiltration characterizes both on biopsy. The progression of a particular phenotype also exhibits differences in latencies. The implicated drugs are infrequently associated with short-latency liver injury, indicating that long latency might also contribute to the evolution of autoimmune features. The imperative, then, is clear: autoantibodies do not establish the diagnosis.

Fig 1 : A comparative panel of mechanisms of AIH, drug-mediated injury, and drug-induced autoimmune hepatitis.
Diagnostic Framework and Its Limitations
The International Autoimmune Hepatitis Group (IAIHG) scoring system and its simplified revision provide a framework for linking specific injury features to the probability of AIH. At the same time, the Roussel Uclaf Causality Assessment Method (RUCAM) operationalizes causality assessment for DILI. Each tool performs coherently in isolation; however, DIAIH presents as a chiasmus of these two frameworks, which, when used together, is more complementary than redundant. A patient may score as “probable AIH” on the IAIHG scale while also achieving a “probable” RUCAM score—a discordance that is not a scoring failure but a reflection of genuine biological overlap. Liver biopsy remains the pivotal arbiter, yet it, too, has limits. The hallmarks of AIH
- Interface hepatitis
- Periportal plasma cell infiltration
- Hepatocyte rosetting
- Emperipolesis

Fig 2 : A comparative histology panel showing various features like rossetting in AIH, centrilobular necrosis in DILI, and overlap in DI-AIH.
But there exists considerable overlap in DI-AIH with substantial frequency. Conversely, centrilobular necrosis, cholestatic injury, and eosinophilic infiltration suggest DILI, but are neither sensitive nor specific. Advanced cirrhosis on biopsy more reliably points towards chronicity of idiopathic AIH, since most of the time DILI resolves without progressive architectural remodeling with acute presentation of liver injury. Still, this criterion fails in patients with delayed diagnosis, multiple drug exposures, or long latencies. Biopsy is pivotal; it is not definitive. A case report by Nnonyelu C highlights the clinician’s dilemma of accurately classifying the phenotype. The fact that anchoring diagnosis to a single cross-sectional data point—serological, histological, or scoring-based—will inevitably misclassify patients at the spectrum’s edges. The diagnostic encounter must be understood as a longitudinal process.
Modern Confounders
The defining feature that separates DI-AIH from idiopathic AIH—sustained remission off immunosuppression after drug cessation—is known only retrospectively, often after months of observation, as supported by the 2019 study by Weber S et al. on the evaluation of disease response to corticosteroid therapy (refer to the figure below). This reaffirms that temporality, the types of interventions, and their responses also serve as diagnostic tools.
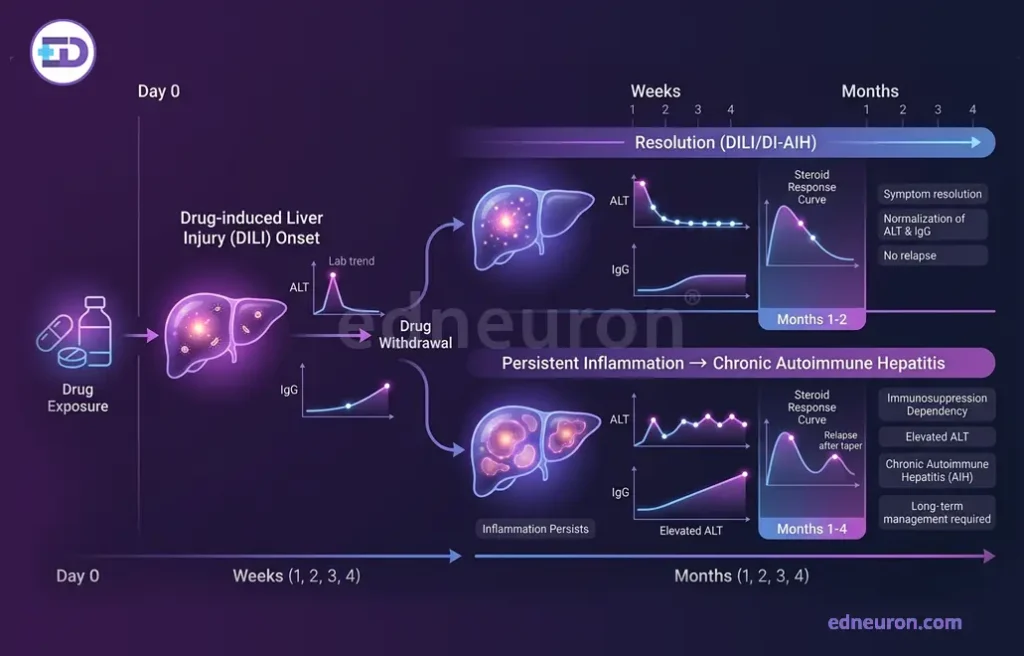
Fig 3 : Illustration of how time works as a diagnostic tool over the course of disease progression.
Another dimension confounding the whole hepatological picture is ICI hepatitis. Programmed death-1 (PD-1) (Pembrolizumab) and CTLA-4 (Ipilimumab) inhibitors used as treatment for metastatic melanoma cause T-cell disinhibition rather than classical autoantigen-driven mechanisms, producing a phenotype that overlaps AIH histologically in terms of panlobular distribution, lymphocytic infiltration, and presence of necrosis, yet typically differs in predominant CD8+ T cell infiltration, different IgG level, autoantibody profile, and temporal relationship to immunosuppression. Crucially, the standard management of ICI hepatitis—high-dose corticosteroids followed by taper—may superficially resemble AIH induction therapy while resting on entirely different immunologic rationale. Conflating ICI hepatitis with idiopathic AIH risks both premature ICI discontinuation and inappropriate long-term immunosuppression in oncology patients who cannot tolerate it.
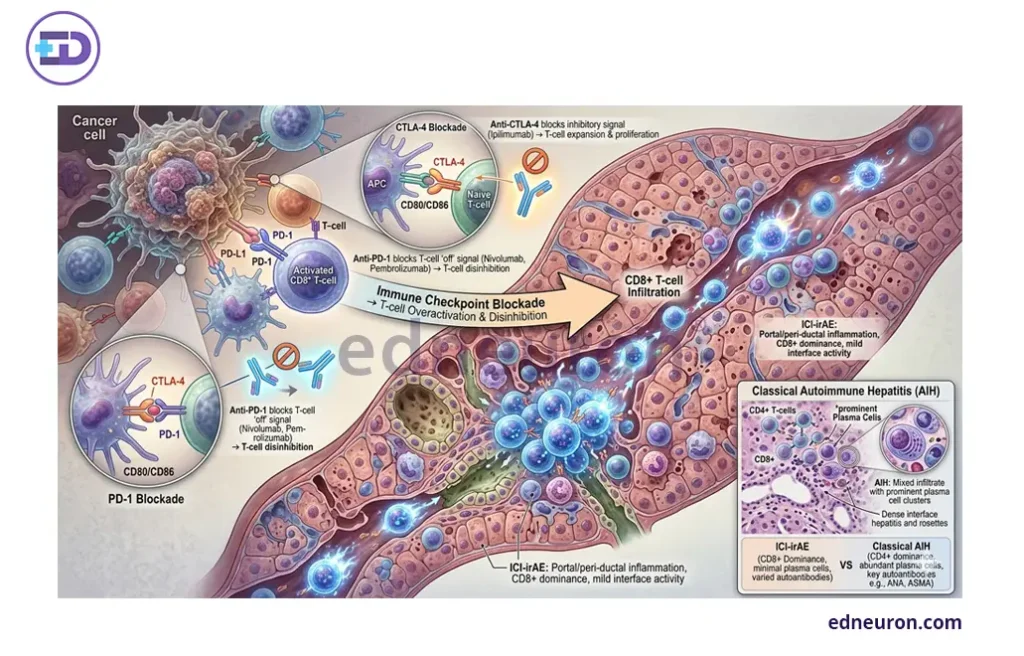
Fig 4 : Immune Checkpoint Inhibitor–Related Hepatitis (ICI-irAE) vs Classical Autoimmune Hepatitis (AIH): Immunopathogenesis and Histologic Features.
Emerging Solution and Future Directions
The search for discriminating biomarkers has recently extended beyond the conventional “plasma cells favor AIH, eosinophils favor DILI” heuristic. Hepatic lipofuscinosis—the accumulation of oxidative stress-derived pigment within hepatocytes—has emerged as a histologic discriminator favoring DILI over AIH in a prospective cohort study (odds ratio [OR] 10.8; positive predictive value [PPV] 96.2%), though poor concordance between histologic and clinical diagnosis in that series underscores how unsettled the field remains. It has been shown that incorporating routine laboratory values, exposure timing, and biopsy features provides greater discriminative power than individual scoring systems alone. However, none have achieved prospective validation or guideline adoption. The 2025 EASL Clinical Practice Guideline update on AIH acknowledges the ever-flexible boundaries of these phenotypic variants and the need for refined histologic standards. What the current standard consistently reaffirms is that no single snapshot or parameter can, in isolation, promise reliable and accurate classification. Longitudinal reassessment—evaluating response to drug withdrawal, immunosuppression, and the durability of remission off treatment—remains the closest approximation to a gold standard the field currently possesses.

Fig 5 : Stepwise evaluation workflow.
Conclusion
The diagnostic encounter at the AIH-DILI interface demands a structured and holistic framework, not just a snapshot of a single diagnostic tool. Autoantibodies are hypothesis-generators, not diagnostic endpoints. Biopsy refines probability but does not adjudicate it. RUCAM and IAIHG scores are complements to clinical reasoning, not substitutes for it. And in the era of immune checkpoint inhibition, the traditional classification schema faces a category of immune-mediated hepatotoxicity that fits neither definition cleanly. The clinical imperative is not to force early diagnostic closure but to build a working hypothesis, initiate the safest management strategy, and revisit the diagnosis as the patient’s course unfolds.
References
- Tan CK, Ho D, Wang LM, Kumar R. Drug-induced autoimmune hepatitis: A minireview. World J Gastroenterol. 2022 Jun PMID: 35979160.
- de Boer YS, Kosinski AS, Urban TJ et al.; Drug-Induced Liver Injury Network. Features of Autoimmune Hepatitis in Patients With Drug-induced Liver Injury. Clin Gastroenterol Hepatol. 2017 Jan PMID: 27311619.
- Moral K, Efe C, Sert A et al. Evaluation of Histological Criteria and Immunoserological Testing of Simplified Criteria for the Diagnosis of Autoimmune Hepatitis. Turk J Gastroenterol. 2025 Sep PMID: 41669943.
- EASL Clinical Practice Guidelines: Drug-induced liver injury. 2019. easl.eu.
- EASL Clinical Practice Guidelines on the management of autoimmune hepatitis. 2025. PubMed: 40348684.
- Nnonyelu C. Diagnostic Dilemma in a Septuagenarian Patient: Drug-Induced Liver Injury (DILI) or Autoimmune Hepatitis? Cureus. 2025 May PMID: 40525045.
- Weber S, Benesic A, Rotter I, Gerbes AL. Early ALT response to corticosteroid treatment distinguishes idiosyncratic drug-induced liver injury from autoimmune hepatitis. Liver Int. 2019 Oct PMID: 31319011..
- Hercun J, Vincent C, Bilodeau M, Lapierre P. Immune-Mediated Hepatitis During Immune Checkpoint Inhibitor cancer Immunotherapy: Lessons From Autoimmune Hepatitis and Liver Immunology. Front Immunol. 2022 Jun PMID: 35844534.
- Weber S, Erhardt F, Neumann J et al. Lipofuscinosis as a novel discriminating feature for drug-induced liver injury from autoimmune hepatitis. Scand J Gastroenterol. 2025 Jun PMID: 40518721.

Author: Aishwarya Prasad
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi


