
Introduction
Most cases of pediatric community-acquired pneumonia (CAP) follow a predictable course, but some children develop complicated community-acquired pneumonia (CCAP), which can lead to issues like parapneumonic effusion, empyema, or necrotizing lung disease. Clinicians must not only recognize the infection but also decide when to shift from medical treatment to more invasive interventions. This creates a challenge between detailed imaging and practical bedside decision-making, especially when resources are limited.
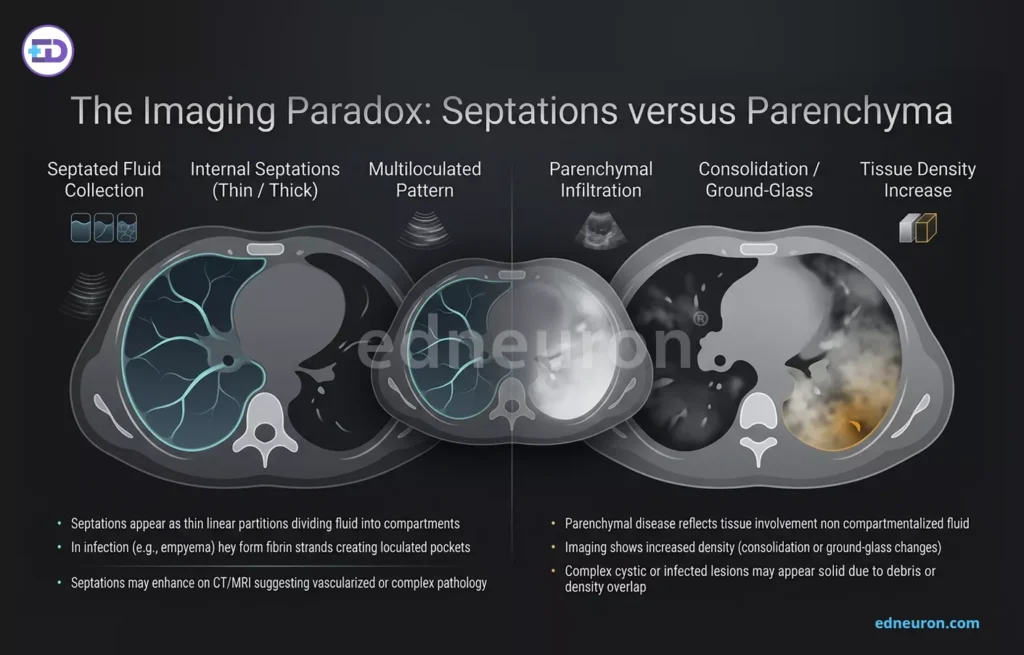
Fig 1: A comparative radiology-style diagram and schematic illustrating the imaging differentiation between septated fluid collections and parenchymal tissue infiltration within the lung.
The Imaging Paradox: Septations versus Parenchyma
Radiographic imaging remains the cornerstone of CCAP management, yet choosing a modality involves a complex trade-off between sensitivity and safety. While contrast-enhanced computed tomography (CT) is historically regarded as the “gold standard” for identifying advanced parenchymal disease, such as consolidation and pulmonary cavities, it exposes pediatric patients to ionizing radiation and requires the logistical hurdle of transporting critically ill children. Conversely, lung ultrasound (LUS) has emerged as a superior tool for the specific characterization of the pleural space.
Studies show that LUS is actually better than CT at detecting fine fibrinous septations in pleural effusions, which can affect whether chest tube drainage will work or if more advanced treatments are needed. Still, CT is important when ultrasound results do not match the clinical picture or if a lung abscess is suspected. This means the best approach is to start with LUS at the bedside and use CT only when more detailed lung images are needed for surgical decisions.
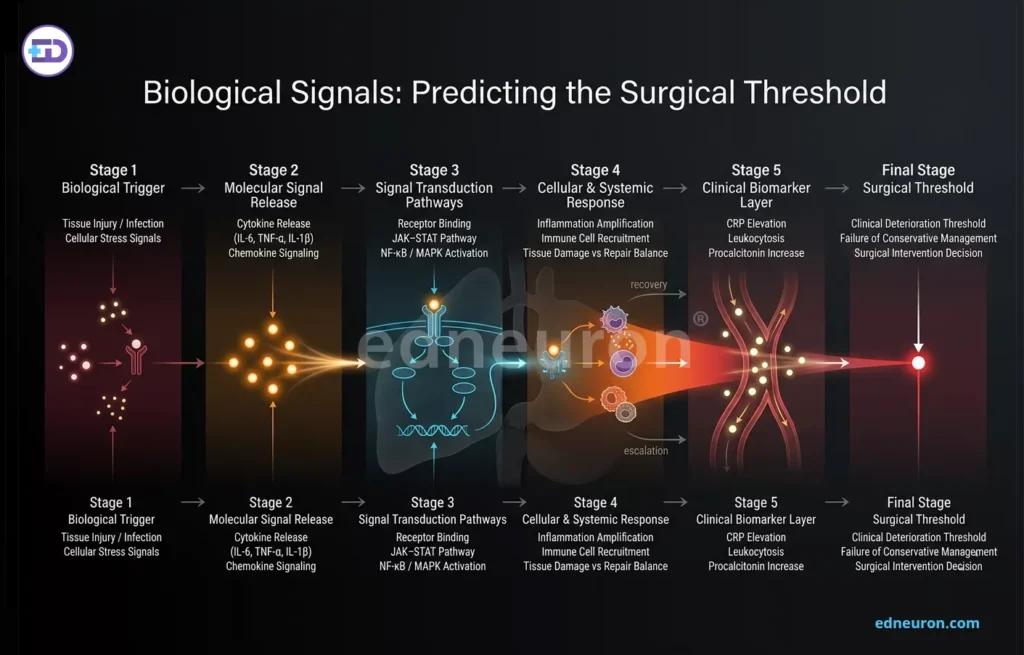
Fig 2: Biological cascade progression: from molecular signals to surgical threshold.
Biological Signals: Predicting the Surgical Threshold
Deciding when to go beyond antibiotics and consider procedures like thoracotomy or video-assisted thoracoscopic surgery (VATS) is often based on clinical judgment. However, new research points to certain biological markers that can help predict when surgery is needed. The Pneumonia Severity Index (PSI) is commonly used to estimate overall risk, but it does not always identify the specific complications that require surgery.
Instead, signs like a pleural peel, which is fibrous tissue that restricts lung movement, and lab findings such as low platelet counts, are strong indicators that surgery may be needed. Thrombocytopenia in these cases often indicates a strong inflammatory response or increased platelet use during severe infection, serving as a warning sign of serious illness. New biomarkers, such as Heparin-Binding Protein (HBP), which is released by activated neutrophils and causes blood vessels to leak, have shown excellent accuracy in detecting severe pneumonia and may be better than traditional markers like C-reactive protein (CRP) for early risk assessment.
Real-World Implications and Global Accessibility
The challenge of diagnosis is compounded when clinical suspicion does not align with imaging findings. Studies show that many children treated for suspected CAP solely on symptoms do not have pneumonia on imaging and often improve, regardless of antibiotic strength. This tendency to overdiagnose in wealthier countries is very different from the situation in low- and middle-income countries, where reaching a well-equipped hospital for severe pneumonia can take a long time.
In these settings, clinical pragmatism dictates that the universal adoption of simple tools, such as pulse oximetry, may be more impactful than pursuing advanced imaging. Identifying hypoxemia early enables timely referral to better-equipped centers, thereby reducing travel time to definitive care.
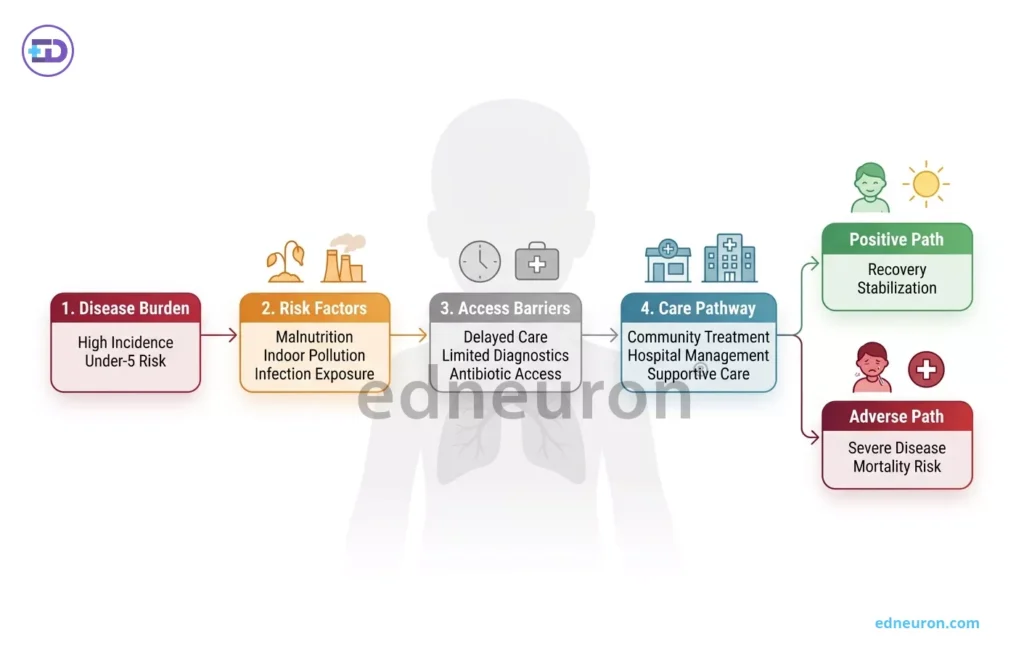
Fig 3: This flowchart illustrates the global pediatric respiratory disease pathway from burden and risk factors to care access and divergent health outcomes.
Conclusion
Complicated pediatric pneumonia demands a diagnostic framework that integrates anatomical imaging, biological signals, and geographical reality. The transition from medical to surgical management should not be triggered by a single finding, but rather by integrating pleural ultrasound findings, biological markers such as HBP or thrombocytopenia, and the patient’s clinical trajectory. Ultimately, resolving the tension in CCAP management requires moving beyond the simple identification of an infiltrate toward a nuanced understanding of the patient’s evolving pathophysiology.
References
- Sharma, R., Gupta, A., & Mehta, P. (2025). Clinical decision-making in pediatric pneumonia: When to operate. Annals of Medicine & Surgery, 89, 104512. Khan, S., Ali, Z., & Rahman, T. (2025). Ultrasonography compared to computed tomography in pediatric complicated pneumonia: Beyond radiation. Cureus, 17(2), e325331.
- Li, Y., Zhang, H., Chen, X., & Wang, J. (2025). Impact of pulmonary infection on thoracoscopic surgery outcomes in children with congenital pulmonary airway malformation. BMC Surgery, 25, 127.
- Smith, L. M., Johnson, K. R., & Patel, N. (2024). Postoperative pneumonia risk in children with neurologic disorders. Hospital Pediatrics, 14(12), 1001–1009.
- Andersson, J., Nilsson, M., & Bergström, S. (2025). Predictive value of heparin-binding protein in pediatric community-acquired pneumonia. Pediatric Research. Advance online publication.
- Zhang, L., Liu, Y., & Chen, Q. (2019). Respiratory virus associated with surgery in pediatric patients. Respiratory Research, 20, 1086.
- Bradley, J. S., & Byington, C. L. (2020). Pneumonia in hospitalized children. Pediatric Clinics of North America, 67(6), 1063–1083.
- McCollum, E. D., Ginsburg, A. S., & Pachl, J. (2022). Resources and geographic access to care for severe pediatric pneumonia. American Journal of Respiratory and Critical Care Medicine, 205(2), 183–195.
- Williams, D. J., Edwards, K. M., & Self, W. H. (2024). Interpretation of antibiotic trials in pediatric pneumonia. JAMA Network Open, 7(1), e2814635.

Author: A D
A surgically inclined medical trainee with a growing interest in brain, spine, and cardiothoracic systems, aspiring to build a career in advanced operative care. He aims to become a patient-centered surgeon who integrates evolving medical technologies with precise clinical judgment. With a strong foundation in surgical sciences, he has gained clinical exposure through case postings involving breast pathologies, chronic ulcers, and diabetic foot, along with observational experience in hernia repair, appendectomy, and cholecystectomy. Academically, he has assisted research work on breast cancer and developed a case report on a complicated hernia surgery, alongside contributing multiple review articles across disciplines. He is currently engaged in ongoing research exploring the role of nutrition in health and disease. MBBS (MS4) GMC Nagpur, India



