
Abstract
Checkpoint inhibitor therapy ushered in a new era in understanding the response assessment in oncological therapeutics. When a patient with advanced non-small cell lung cancer (NSCLC) receiving nivolumab demonstrates 35% primary lesion enlargement and two new pulmonary nodules at first restaging, RECIST 1.1 mandates a determination of progressive disease. iRECIST allows for a non-definitive window period, i.e., unconfirmed progressive disease (iUPD), permitting a 4–8-week confirmatory interval. This article examines the redundancy of relying on radiographic modalities in isolation for assessing biological function. Apart from modifications made in RECIST 1.1 to standardize the interpretation of clinical trials data, there must also be pronounced integration of imaging, tumor growth kinetics, circulating tumor DNA (ctDNA) dynamics, symptom trajectory, and ECOG performance status in real time as surrogate markers for tumor burden, thereby also assessing quality of life. The central diagnostic dilemma revolves around three competing differential diagnoses which need to be assessed in parallel: pseudoprogression driven by immune-cell infiltration, true progressive disease reflecting therapeutic resistance, and hyperprogressive disease (HPD): a paradoxical, clinically perilous acceleration of tumor growth following checkpoint blockade. Finding that demarcating line with a single snapshot rather than a longitudinal study can be really challenging, as each scenario correlates with varied kinetic signatures, distinct biomarker correlates, and markedly different clinical urgency, while explicitly acknowledging that no universally validated decision algorithm currently exists.
Clinical Case
A 67-year-old male with stage IVB PD-L1–high tumor proportion score (TPS 80%) non-small cell lung adenocarcinoma without any driver mutations that can be targeted, initiates nivolumab monotherapy. First restaging CT at an interval of 6 weeks demonstrates:
- The primary right upper lobe lesion has +35% increase in the longest diameter.
- Two new bilateral pulmonary nodules (6 mm and 8 mm)
- No new extrathoracic disease
- RECIST 1.1 Progressive Disease (PD)-threshold met; new lesions confirm progression.
- iRECIST categorizes as immune Unconfirmed Progressive Disease (iUPD)-confirmatory scan recommended in 4–8 weeks.
- ECOG PS 1. Patient has stable symptoms, no new oxygen requirement, no cachexia, and CTDNA result pending.
Central question: Can this patient safely continue nivolumab pending confirmatory imaging?
The Interpretation of Radiological Images and their Discontents
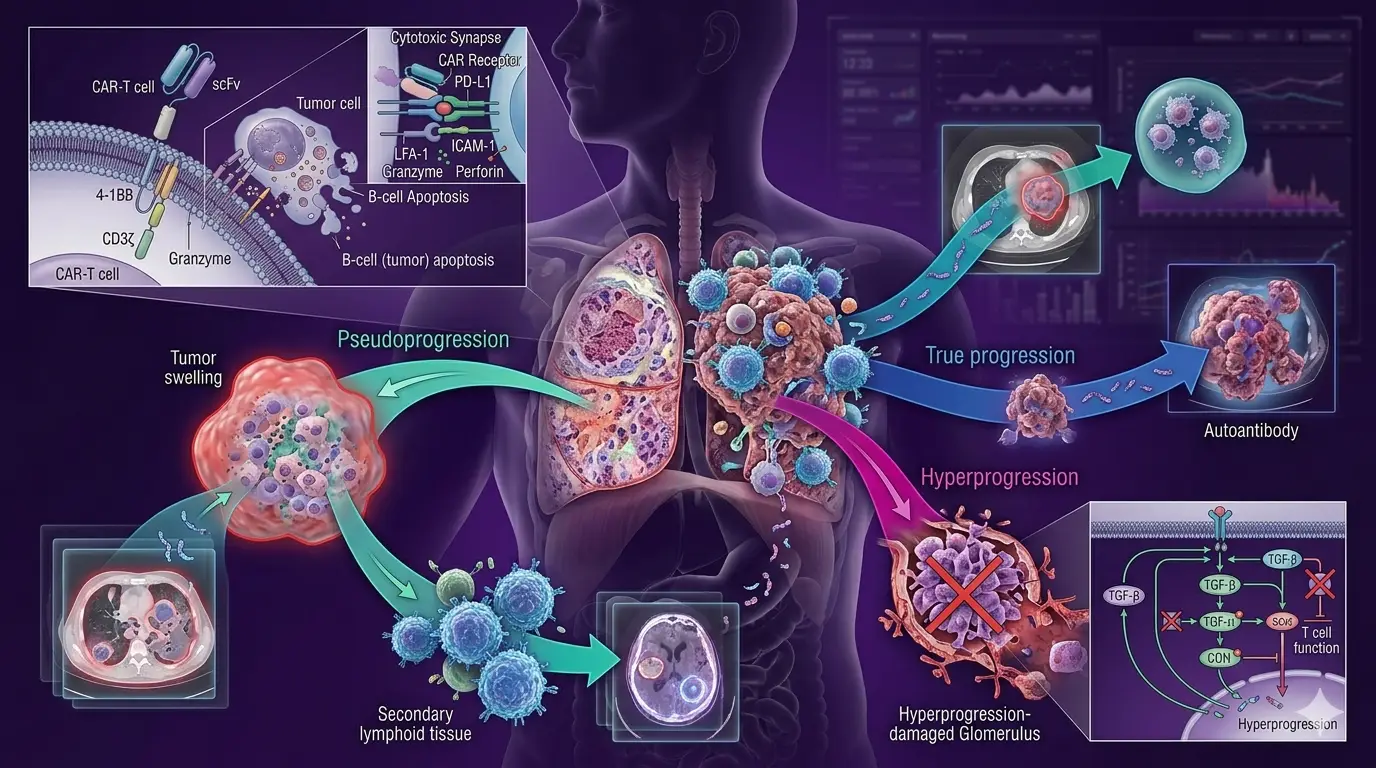
Oncology has built its response assessment language model around anatomy. The RECIST 2000 working committee operationalized tumor burden legibility through size, with shrinkage as a meaningful clinical endpoint (size reductions serving as surrogates for clinical efficacy). Progressive disease is geometrically assessed: a 20% increase in the sum of target lesion diameters, or the appearance of new lesions, indicates that treatment has failed and a new strategy is required. In the earlier times of cytotoxic chemotherapy, this presumption was largely defensible. Tumor growth under chemotherapy meant drug resistance, and continued exposure offered little except toxicity. Checkpoint inhibitor therapy dismantled this logic without immediately replacing it. The mechanism of PD-1/CTLA-4 immune therapies differs from cytotoxic killing in the sense that it restores T-cell surveillance capacity and enables the immune system to orchestrate a delayed-onset, inflammatory cytotoxic response with potentially durable effects. (refer to Fig 1)
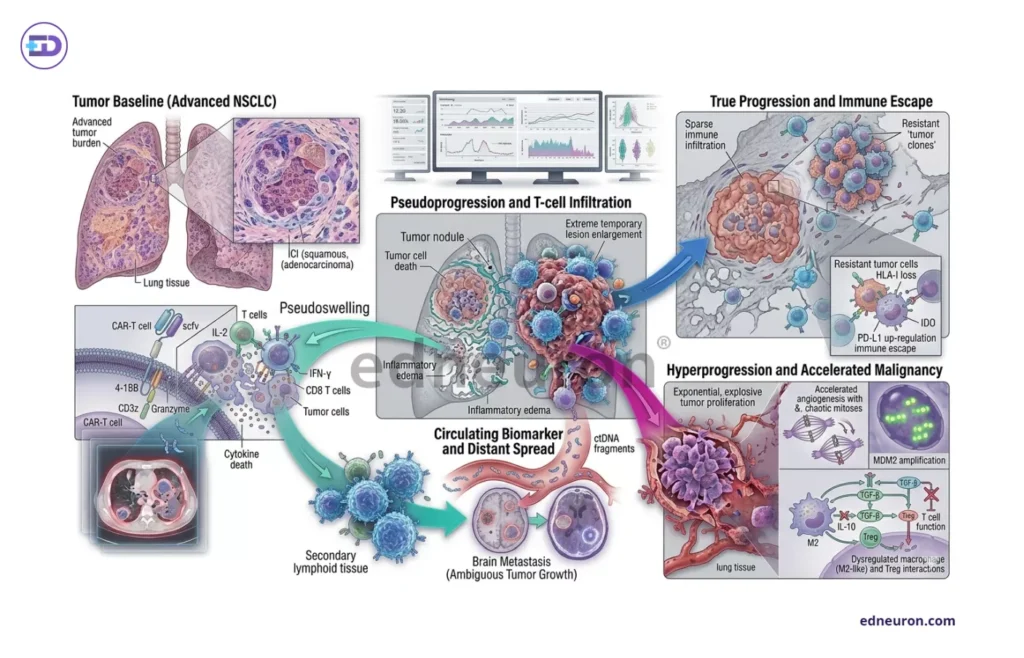
Fig 1 : Outcome in checkpoint inhibitor therapy vs true progression of disease.
Wolchok and colleagues formalized what had been observed by practicing clinicians, i.e., radiographic worsening during immunotherapy could precede meaningful clinical benefit, and that criteria designed for chemotherapy could not be applied without modification. iRECIST, codified by Seymour and the RECIST working group in 2017, went further and defined efficacy endpoint that incorporates unconfirmed progressive disease as an explicit operational acknowledgment, with progression under immunotherapy to be treated as probabilistic rather than absolute. However, these efforts were aimed at establishing uniform global standards for data warehouses and clinical trial results, enabling meaningful analysis and interpretation. Our patient, whose imaging satisfies RECIST 1.1 criteria for progressive disease, presents precisely with this problem. It also satisfies the iRECIST criteria for iUPD. The two frameworks agree on what the scan shows; they disagree fundamentally on what it means. The resolution of that disagreement is not radiographic. It is biological.
What iRECIST Ameliorates that RECIST does not
Unlike cytotoxic clearance, post-therapy tumor flare, in the form of new nodules/exorbitant increase in the expected size, represents immune trafficking events and precedes any clinical benefit, as checkpoint inhibitors uncouple tumor burden from size. Imaging becomes temporally discordant with the underlying immune response dynamics. iRECIST does not solve this problem; it acknowledges it. The introduction of iUPD recognizes that the first post-immunotherapy scan cannot be read as definitively as a chemotherapy response assessment. But iRECIST offers a window, not a verdict. The biological question of what is happening within that window (immune flare, resistance, or acceleration) remains the physician’s problem to solve.
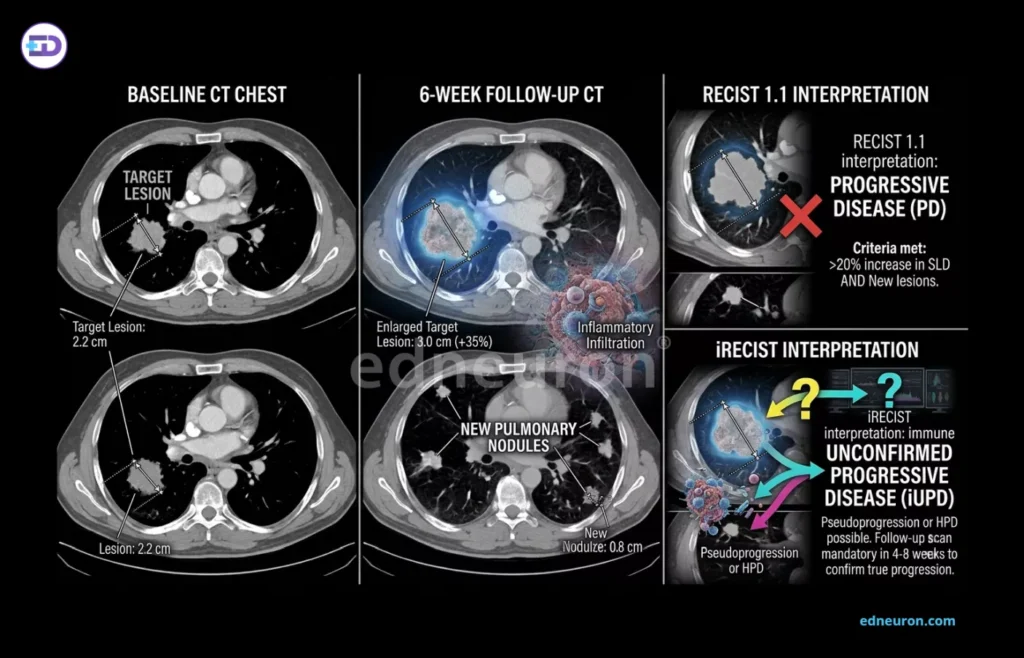
Fig 2 : Comparative panel of radiologic illustration and different inference by RECIST 1.1 vs iRECIST.
Three Competing Consequences
The following three phenomena, with imaging signatures indistinguishable from one another after the designated 4-8 week interval, have implications that are worlds apart, requiring prompt decision-making and apt recognition.
- Pseudoprogression manifests as transient radiographic enlargement due to immune-cell infiltration and inflammatory edema. The absolute incidence of radiographic pseudoprogression is estimated at 3–5% among patients with NSCLC who appear to progress on initial imaging. While clinically meaningful, such data imply that for every patient with pseudoprogression, the vast majority of apparent early progressors have true disease progression. Indiscriminate continuation of therapy in the expectation of delayed response would expose most patients to the risks of untreated progressive disease, or worse, to hyperprogression during the observation window.
- True progressive disease: clonal tumor expansion driven by intrinsic or acquired resistance to PD-1 axis disruption.
- Hyperprogressive disease is a paradoxical acceleration of tumor growth/kinetic phenomenon in which the tumor growth rate (TGR) or tumor growth kinetics (TGK) on therapy substantially exceeds the pre-treatment growth trajectory. The leading hypotheses underlying the mechanism point to impaired Treg function, macrophage-mediated immune dysregulation, and aberrant Fc-receptor signaling triggered by PD-1 antibody binding, which, rather than suppressing tumor growth, instead aberrantly supports it. It has also been shown that MDM2/MDM4 amplifications are associated with an increased risk of hyperprogressive disease, and that EGFR alterations (upregulation of PD-1/PD-L1 or CTLA-4) are associated with tumor immune escape and explosive post-ICI kinetics in certain cohorts. These associations have not been consistently reproduced, and no genomic signature can be considered a reliable predictor of prospective HPD. However, what is validated retrospectively may be the clinical consequence that a confirmatory imaging interval may prove to be catastrophic for patients who hyperprogress.
In the context of our patient, the 4–8 weeks permitted by iRECIST before a confirmatory scan is not a neutral waiting period; it is an interval during which explosive tumor acceleration may render subsequent therapeutic options inaccessible. This asymmetry of risk: pseudoprogression is recoverable if therapy continues; HPD during observation may not be, is the central ethical tension in the checkpoint-era progression problem. iRECIST provides a temporal framework; it does not resolve the biological question of which trajectory a given patient is on.
ctDNA as a near-real-time evolutionary biomarker
The advent of a new monitoring tool, circulating tumor DNA dynamics, offers, at least in theory, what imaging fails to provide: a near-real-time molecular readout of clonal tumor behavior that is not entangled by an inflammatory mass. The more tumor cells die, the more ctDNA is disseminated, with its kinetics under therapy foreshadowing the radiographic response in the coming weeks, thus providing an aid in monitoring the tumor’s clonal architecture: whether it is contracting, stable, or expanding. The clinical framework is in its nascent stages and, although not yet universally validated, is instructive. A patient whose ctDNA drops by more than 50% from baseline during the iUPD interval, despite radiographic imaging showing tumor enlargement, presents a coherent signature of pseudoprogression. The dichotomy is that even when the tumor is dying at the molecular level, inflammation produces quantifiable changes in size. Conversely, in a patient whose ctDNA rises three-fold or more during the same interval, it insinuates clonal expansion, making the diagnosis of HPD or true progression highly likely and continued therapy potentially dangerous. Despite the propitious prospects, there must be an iron-clad framework to infer standardized ctDNA from which will help govern the continuation or cessation of immunotherapy, as long as the current system lacks an FDA-approved threshold value. The existing evidence base remains largely retrospective and analytically heterogeneous across platforms and tumor types.
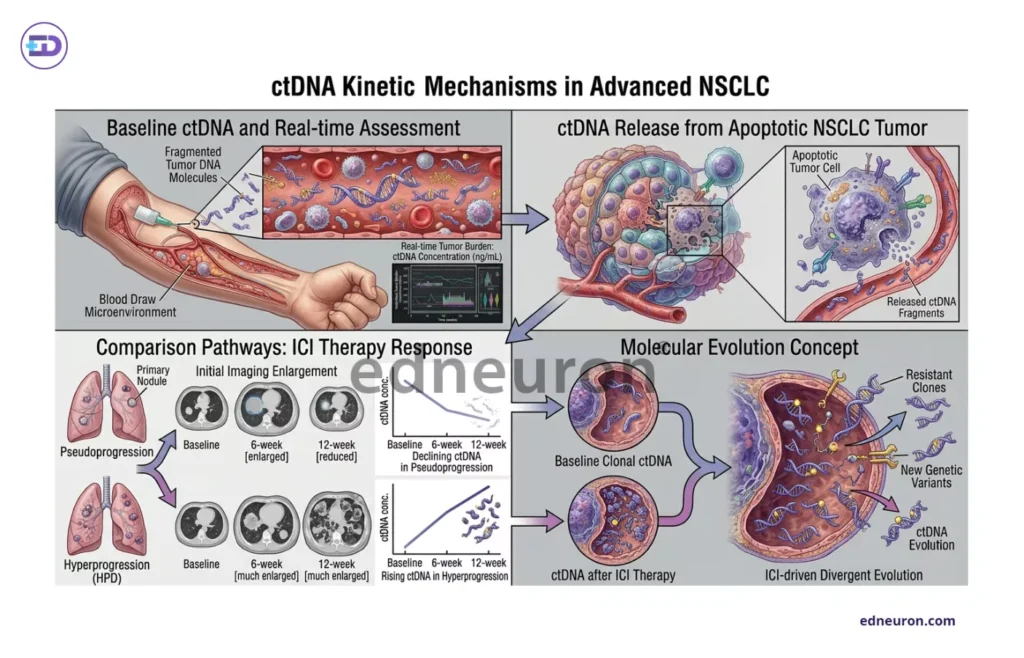
Fig 3 : ctDNA kinetics in advanced NSCLC.
Clinical Judgment as the Integrating Faculty
- A patient at ECOG PS 1 (restricted in strenuous activity but ambulatory and able to do light work) who is clinically stable at 6 weeks, with maintained oxygen saturation, stable or reduced symptom burden, and no acceleration of weight loss/pain, is more likely to have a pseudo-progressive pattern or a stable disease.
- Conversely, a patient requiring increased oxygen supply with dyspnea/cachexia, and profound deterioration during the 4 weeks or after the relapse window should raise immediate suspicions about HPD or aggressive true progression.
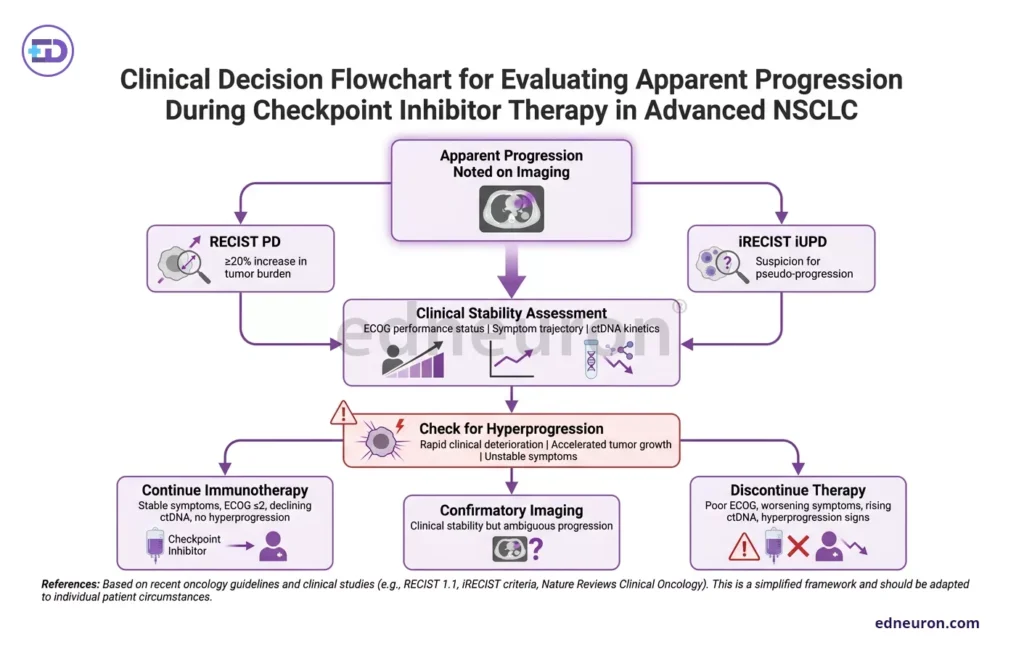
Fig 3 : Evaluation strategy..
Two patients with similar 4-week imaging findings can end up on completely different trajectories depending on the ctDNA burden and MDM alterations in their genomic profiles. This, in itself, is an extended reflection that immunotherapy response assessment is fundamentally an uncertainty-management problem and requires integrative reasoning and longitudinal interpretation rather than algorithmic substitution, thereby superseding static imaging in translational oncology assessment.
References
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, Kaplan R, Lacombe D, Verweij J. New response evaluation criteria in solid tumors: revised RECIST guideline (version 1.1). Eur J Cancer. 2009 Jan;45(2):228-47. doi: 10.1016/j.ejca.2008.10.026. PMID: 19097774.
- Wolchok JD, Hoos A, O’Day S et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res. 2009 Dec 1;15(23):7412-20. PMID: 19934295.
- Kato S, Goodman A, Walavalkar V et al. Hyperprogressors after Immunotherapy: Analysis of Genomic Alterations Associated with Accelerated Growth Rate. Clin Cancer Res. 2017 Aug 1;23(15):4242-4250. PMID: 28351930.
- Shen P, Han L, Ba X, Qin K, Tu S. Hyperprogressive Disease in Cancers Treated With Immune Checkpoint Inhibitors. Front Pharmacol. 2021 Jul 5;12:678409. PMID: 34290608
- Zhang Q, Luo J, Wu S et al. Prognostic and Predictive Impact of Circulating Tumor DNA in Patients with Advanced Cancers Treated with Immune Checkpoint Blockade. Cancer Discov. 2020 Dec;10(12):1842-1853. PMID: 32816849.
- Al-Showbaki L, Wilson B, Tamimi F et al. Changes in circulating tumor DNA and outcomes in solid tumors treated with immune checkpoint inhibitors: a systematic review. J Immunother Cancer. 2023 Feb;11(2):e005854. PMID: 36792122.

Author: A P
A medical trainee with an emerging focus on translational and clinical research, with interests spanning surgical sciences, neuroscience, pediatrics, and immunology. Her academic trajectory reflects an effort to integrate molecular innovation with clinically relevant disease models, particularly in complex and high-burden conditions. Her research experience includes work in genome engineering, specifically in prime editing, exploring its therapeutic potential in precision medicine. She has also contributed to oncological research examining cholangiocarcinoma with brain metastasis, focusing on its clinical course and diagnostic challenges. In parallel, her work investigating stoma formation as an independent risk factor for acute kidney injury reflects an interest in perioperative and systemic complications. Academically, she has contributed to case-based and review-driven scholarship, including a case reports and interdisciplinary review articles. Her evolving interests in neurology, pediatrics, and immunology reflect a broader inclination toward understanding disease across systems—from molecular mechanisms to clinical outcomes—while maintaining a disciplined, evidence-based approach to patient care. MBBS (MS4) ABVIMS Dr. RML HOSPITAL New Delhi



